You might also like
- Management of StutteringDocument182 pagesManagement of Stutteringpappu713100% (2)
- Premature Dropout From Psychotherapy Prevalenc, Perceived Reasons and Consequences As Rated by CliniciansDocument16 pagesPremature Dropout From Psychotherapy Prevalenc, Perceived Reasons and Consequences As Rated by CliniciansMichelle KellyNo ratings yet
- Paper Salud FamiliarDocument7 pagesPaper Salud FamiliarLucas Braga Almeida e SilvaNo ratings yet
- Description of Dementia Caregiver Uplifts and Implications For Occupational TherapyDocument6 pagesDescription of Dementia Caregiver Uplifts and Implications For Occupational TherapyKimmy ChuNo ratings yet
- RecognitionDocument22 pagesRecognitionPalomaNo ratings yet
- Efficacy of Stuttering Therapies - PDF /KUNNAMPALLIL GEJODocument24 pagesEfficacy of Stuttering Therapies - PDF /KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNo ratings yet
- CABG Discharge Planning 1Document16 pagesCABG Discharge Planning 1pipporudyNo ratings yet
- The Compliance Following Medical AdviceDocument37 pagesThe Compliance Following Medical AdviceAamna HaneefNo ratings yet
- Research Assessing Consumer Satisfaction With Mental Health T Atment: A Review of FindingsDocument26 pagesResearch Assessing Consumer Satisfaction With Mental Health T Atment: A Review of FindingsFanni VikorNo ratings yet
- Evaluating Inpatient Satisfaction With A Physiotherapy Service: A Rehabilitation Centre SurveyDocument10 pagesEvaluating Inpatient Satisfaction With A Physiotherapy Service: A Rehabilitation Centre SurveygabrimarteNo ratings yet
- Recognition of Psychotherapy EffectivenessDocument14 pagesRecognition of Psychotherapy EffectivenessÍcaro VieiraNo ratings yet
- ACT Vs CBT For GADDocument22 pagesACT Vs CBT For GADalvarogmc02No ratings yet
- Effectiveness of Psychotherapeutic Treatment: Michael J. LambertDocument14 pagesEffectiveness of Psychotherapeutic Treatment: Michael J. LambertGerson De La FuenteNo ratings yet
- 2009 01follow UpOutcomeinShort TermGroupTherapyforComplicatedGriefDocument14 pages2009 01follow UpOutcomeinShort TermGroupTherapyforComplicatedGriefrobertd33No ratings yet
- Intensive Stuttering Modification Therapy: A Multidimensional Assessment of Treatment OutcomesDocument18 pagesIntensive Stuttering Modification Therapy: A Multidimensional Assessment of Treatment OutcomesDobrovski PetroviciNo ratings yet
- Swift y Greenberg. (2012) .Premature Discontinuation in Adult Psychotherapy. A Meta-AnalysisDocument13 pagesSwift y Greenberg. (2012) .Premature Discontinuation in Adult Psychotherapy. A Meta-AnalysisDiego Martinez SantanaNo ratings yet
- Efectividad de La Terapia en Adolescentes Con TartamudezDocument14 pagesEfectividad de La Terapia en Adolescentes Con TartamudezcynthiaNo ratings yet
- Effectiveness of Intensive, Group Therapy For Teenagers Who StutterDocument14 pagesEffectiveness of Intensive, Group Therapy For Teenagers Who StutterMinkushNo ratings yet
- Slipping Through the Cracks: Intervention Strategies for Clients with Multiple Addictions and DisordersFrom EverandSlipping Through the Cracks: Intervention Strategies for Clients with Multiple Addictions and DisordersNo ratings yet
- Stages of Change and Stuttering: A Preliminary View: Jennifer Floyd, Patricia M. Zebrowski, Gregory A. FlammeDocument26 pagesStages of Change and Stuttering: A Preliminary View: Jennifer Floyd, Patricia M. Zebrowski, Gregory A. Flammemajid mirzaeeNo ratings yet
- What Cognitive Behavioral Techniques Do Therapists Report Using When Delivering Cognitive Behavioral Therapy For The Eating DisordersDocument6 pagesWhat Cognitive Behavioral Techniques Do Therapists Report Using When Delivering Cognitive Behavioral Therapy For The Eating DisordersMihaela-Claudia NedelceaNo ratings yet
- Sense-Making, Grief, and The Experience of Violent Loss Toward A Mediational ModelDocument5 pagesSense-Making, Grief, and The Experience of Violent Loss Toward A Mediational ModelSilvana ArendNo ratings yet
- Using Occupation To Facilitate Self-Awareness in People Who Have Acquired Brain Injury: A Pilot StudyDocument12 pagesUsing Occupation To Facilitate Self-Awareness in People Who Have Acquired Brain Injury: A Pilot StudyDanonino12No ratings yet
- Wong Et Al-2015-Health & Social Care in The CommunityDocument13 pagesWong Et Al-2015-Health & Social Care in The CommunityJoNo ratings yet
- Post-Seclusion And/or Restraint Review in Psychiatry: A Scoping Review Article OutlineDocument27 pagesPost-Seclusion And/or Restraint Review in Psychiatry: A Scoping Review Article OutlineStudentnurseMjNo ratings yet
- Detailed NotesDocument18 pagesDetailed NotesAleeza MalikNo ratings yet
- The Question of Expertise in PsychotherapyDocument9 pagesThe Question of Expertise in PsychotherapyAnonymous aCmwhRdNo ratings yet
- IMRAD Format2Document33 pagesIMRAD Format2Juvy IringanNo ratings yet
- Assessing Patient Suitability For ShortDocument16 pagesAssessing Patient Suitability For ShortoflynnjenniferNo ratings yet
- Piper (2001)Document28 pagesPiper (2001)Carla ServínNo ratings yet
- Expert Guidance: Head and Neck Cancer DysphagiaDocument3 pagesExpert Guidance: Head and Neck Cancer DysphagiaSpeech & Language Therapy in PracticeNo ratings yet
- Factors Influencing Compliance With Home Exercise Programs Among Patients With Upper-Extremity ImpairmentDocument10 pagesFactors Influencing Compliance With Home Exercise Programs Among Patients With Upper-Extremity ImpairmentVanesaNo ratings yet
- Evidence in Support of Periodontal Therapy-End PointsDocument31 pagesEvidence in Support of Periodontal Therapy-End PointsMohammad HarrisNo ratings yet
- Factors For Personal CounselingDocument12 pagesFactors For Personal CounselingRashika JayakumarNo ratings yet
- Assessing Patient Suitability For Short-Term Cognitive Therapy With An Interpersonal FocusDocument17 pagesAssessing Patient Suitability For Short-Term Cognitive Therapy With An Interpersonal FocuslindsaydicksonNo ratings yet
- MET and Methamphetamine UseDocument8 pagesMET and Methamphetamine UsepoopmanNo ratings yet
- Federici 2007Document10 pagesFederici 2007Tomáš MartínekNo ratings yet
- First Session Solution-Focused Brief Therapy With PDFDocument24 pagesFirst Session Solution-Focused Brief Therapy With PDFMasniahNo ratings yet
- Health Assessment ChristianDocument23 pagesHealth Assessment ChristianNikky Rossel FloresNo ratings yet
- A New Cognitive Behavioural Approach To The Treatment of Obesity - Cooper and Fairburn, 2001Document13 pagesA New Cognitive Behavioural Approach To The Treatment of Obesity - Cooper and Fairburn, 2001Anonymous NvqeV7cNo ratings yet
- Patient Adherence To Medical Treatment A Meta ReviewDocument142 pagesPatient Adherence To Medical Treatment A Meta ReviewVictor MNNo ratings yet
- Evidence-Based Treatment of StutteringDocument10 pagesEvidence-Based Treatment of Stutteringmajid mirzaeeNo ratings yet
- Ebp PresentationDocument21 pagesEbp Presentationapi-336440650No ratings yet
- Treatment Recommendation in Vietnamese Medical Consultations (Final)Document19 pagesTreatment Recommendation in Vietnamese Medical Consultations (Final)Global Research and Development ServicesNo ratings yet
- Chap 7 Health PsychDocument11 pagesChap 7 Health PsychFahmi RifaldiNo ratings yet
- Advances in Management of Stuttering by KunnampallilDocument47 pagesAdvances in Management of Stuttering by KunnampallilKUNNAMPALLIL GEJO JOHNNo ratings yet
- Psychology and Health Notes - CIE Psychology A-LevelDocument18 pagesPsychology and Health Notes - CIE Psychology A-LevelRajasekar KrishnasamyNo ratings yet
- Insomnia 1Document18 pagesInsomnia 1Ria AngganiNo ratings yet
- Licenciatura en Psicología: Cd. Victoria, Tam. Febrero de 2014Document17 pagesLicenciatura en Psicología: Cd. Victoria, Tam. Febrero de 2014Denisse ChaconNo ratings yet
- Models of Health BehaviorDocument81 pagesModels of Health BehaviorFrench Pastolero-ManaloNo ratings yet
- A 3-Year Patient-Centred Follow-Up of 516 Consecutively Treated Orthognathic Surgery PatientsDocument7 pagesA 3-Year Patient-Centred Follow-Up of 516 Consecutively Treated Orthognathic Surgery Patientsodontologia uvNo ratings yet
- Telephone-Delivered Acceptance and Commitment TherDocument6 pagesTelephone-Delivered Acceptance and Commitment TherMaria Luisa Barreto ZambranoNo ratings yet
- CBT Clinical Perfeccionism (Fairburn)Document11 pagesCBT Clinical Perfeccionism (Fairburn)Admi PigmalionNo ratings yet
- Healthier Lifestyle, Behaviour ChangeDocument4 pagesHealthier Lifestyle, Behaviour ChangeupelworopezaNo ratings yet
- AddictionDocument7 pagesAddictionWilly TanNo ratings yet
- TRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNDocument50 pagesTRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNKUNNAMPALLIL GEJO JOHN100% (5)
- (UNIDAD 4) Prochaska Et Al 1992 Am PsycholDocument13 pages(UNIDAD 4) Prochaska Et Al 1992 Am PsycholCintia CoassoloNo ratings yet
- Why Patients Do Not Adhere To Medical Advice.: Health PsychologyDocument109 pagesWhy Patients Do Not Adhere To Medical Advice.: Health PsychologyNie' MK100% (1)
- Cricitical Journal Review 'Educational Psychology': Lecture: Prof. Dr. Ibnu Hajar, M.Si. Rizki Ramadhan S.PD, M.PDDocument21 pagesCricitical Journal Review 'Educational Psychology': Lecture: Prof. Dr. Ibnu Hajar, M.Si. Rizki Ramadhan S.PD, M.PDRahma disaNo ratings yet
- Assesel 1 First MeetingDocument10 pagesAssesel 1 First MeetingNORALYN VELASCONo ratings yet
- Office of The RegistrarDocument1 pageOffice of The RegistrarMarlon Kerwin Ramos CalmerinNo ratings yet
- Significance of The Study Architectural Thesis SampleDocument8 pagesSignificance of The Study Architectural Thesis Samplefbyx8sck100% (1)
- What Is Subject Verb AgreementDocument3 pagesWhat Is Subject Verb AgreementMarkNo ratings yet
- TJC Community: Leadership ProgrammeDocument18 pagesTJC Community: Leadership ProgrammeMelissa TeoNo ratings yet
- Lpe2301 Academic Interaction & Presentation SEMESTER 1, 2019/2020 Lecture Notes 2 (Week 2 - 6)Document8 pagesLpe2301 Academic Interaction & Presentation SEMESTER 1, 2019/2020 Lecture Notes 2 (Week 2 - 6)Hoh Jia DaNo ratings yet
- TVE - EP7-8 - Week 3Document4 pagesTVE - EP7-8 - Week 3via gepilaNo ratings yet
- Explanatory Models and Practice Models of SHRDDocument5 pagesExplanatory Models and Practice Models of SHRDSonia TauhidNo ratings yet
- There Will Come Soft Rains. Lesson - AnthologyDocument14 pagesThere Will Come Soft Rains. Lesson - AnthologydogNo ratings yet
- List of TextbooksDocument5 pagesList of TextbooksESPORTS GAMING ZONENo ratings yet
- Olugbenga's CV EngineerDocument2 pagesOlugbenga's CV EngineerSanni Tajudeen OlugbengaNo ratings yet
- A Century of Social Psychology PDFDocument21 pagesA Century of Social Psychology PDFMarcia JohnssonNo ratings yet
- Lessons From Good Language Learner Part2 ContentsDocument3 pagesLessons From Good Language Learner Part2 ContentsMegabiteUQNo ratings yet
- Chap03 (1) With Answers PDFDocument76 pagesChap03 (1) With Answers PDFNihalAbou-GhalyNo ratings yet
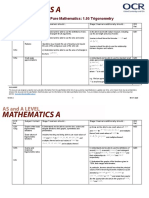
- Teacher Delivery Guide Pure Mathematics: 1.05 TrigonometryDocument16 pagesTeacher Delivery Guide Pure Mathematics: 1.05 TrigonometryHubert SelormeyNo ratings yet
- Stress and Anxiety: Essay SampleDocument3 pagesStress and Anxiety: Essay SampleAshley Jane MacapayadNo ratings yet
- HRD-QOHSER-002 Application FormDocument7 pagesHRD-QOHSER-002 Application FormMajestik ggNo ratings yet
- Software Development Plan TemplateDocument5 pagesSoftware Development Plan TemplateArvada Solutions0% (1)
- EE423 Syllabus Teaching Plan Spring 2012GDocument2 pagesEE423 Syllabus Teaching Plan Spring 2012Gsurendar147No ratings yet
- Project NEXT Accomplishment ReportDocument5 pagesProject NEXT Accomplishment ReportRodolfo NelmidaNo ratings yet
- Books - MY - JOURNEY - IN - SCIENCE - Autobiography - of - An Indian Scientist - Hardev Singh Virk PDFDocument216 pagesBooks - MY - JOURNEY - IN - SCIENCE - Autobiography - of - An Indian Scientist - Hardev Singh Virk PDFHarjinder Singh DhaliwalNo ratings yet
- Facilitating Learning - Module 3Document171 pagesFacilitating Learning - Module 3Rema MandaNo ratings yet
- English ProjectDocument15 pagesEnglish Projectpranit.saluja.ps.2324No ratings yet
- Income Certificate Format - 2021Document1 pageIncome Certificate Format - 2021Faltu Ka jhamlqNo ratings yet
- So MKT205 PDFDocument17 pagesSo MKT205 PDFak shNo ratings yet
- Broadcaster 2012 89-2 WinterDocument25 pagesBroadcaster 2012 89-2 WinterConcordiaNebraskaNo ratings yet
- Role of Teachers in Imparting Value EducationDocument3 pagesRole of Teachers in Imparting Value EducationMehebub AlamNo ratings yet
- Health Teaching For Development MilestonesDocument9 pagesHealth Teaching For Development MilestonesZen PingawanNo ratings yet
- 3rd Faculty MeetingDocument7 pages3rd Faculty MeetingHeidie BalabboNo ratings yet