You might also like
- Common Sports InjuryDocument71 pagesCommon Sports InjuryGlen Dizon100% (1)
- Rife Consolidated Annotated Frequency List - EMR Labs, LLCDocument19 pagesRife Consolidated Annotated Frequency List - EMR Labs, LLCMatimba SimangoNo ratings yet
- Ameloblastoma: DR - Ansar Uddin Ahmed Asst. Prof and Head Periodontology, Oral Pathology and Oral MedicineDocument33 pagesAmeloblastoma: DR - Ansar Uddin Ahmed Asst. Prof and Head Periodontology, Oral Pathology and Oral MedicineTas DidNo ratings yet
- Odontogenic Tumors4Document69 pagesOdontogenic Tumors4LuthfieHaqNo ratings yet
- 11.odontogenic TumorsDocument93 pages11.odontogenic TumorsAyesha Younas100% (1)
- Odontogenic Tumours - (2) L5Document28 pagesOdontogenic Tumours - (2) L5nooraaaNo ratings yet
- Odontogenic Tumors of Oral Cavity: Dr. Deepak K. GuptaDocument44 pagesOdontogenic Tumors of Oral Cavity: Dr. Deepak K. GuptaBinek NeupaneNo ratings yet
- Odontogenic Tumor PDFDocument93 pagesOdontogenic Tumor PDFEmad Alriashy100% (1)
- Heart BlockDocument26 pagesHeart BlockTrending raze100% (1)
- Benign Odontogenic Tumors of Jaws (AmeloblastomaDocument70 pagesBenign Odontogenic Tumors of Jaws (Ameloblastomagalina poberezhnikNo ratings yet
- Oncology: Study of TumorsDocument32 pagesOncology: Study of TumorsGeorge CherianNo ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Pathology McqsDocument130 pagesPathology McqsMotasem Othman67% (3)
- Odontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37Document73 pagesOdontogenic Tumor Ameloblastoma: Presented By: Ankita Singh Bds Final Year Roll No 37ankita sethiNo ratings yet
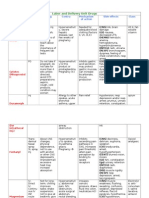
- Maternity DrugsDocument8 pagesMaternity Drugsjanet rooseveltNo ratings yet
- Bronchopneumonia Case PresentationDocument17 pagesBronchopneumonia Case Presentationgandhialpit100% (1)
- Research ProposalDocument17 pagesResearch Proposalapi-297065332No ratings yet
- Odontogenic TumorsDocument14 pagesOdontogenic Tumorskavin_sandhuNo ratings yet
- Radiographic Tumors PDFDocument58 pagesRadiographic Tumors PDFRiskha Febriani HapsariNo ratings yet
- Primary PreventionDocument2 pagesPrimary Preventionsurviving nursing schoolNo ratings yet
- Uterine MYOMADocument5 pagesUterine MYOMARoss Manalang100% (2)
- Imci QuestionDocument21 pagesImci Questionmesdejen75% (12)
- Disorders of The Nervous SystemDocument5 pagesDisorders of The Nervous SystemAgronaSlaughterNo ratings yet
- H MoleDocument7 pagesH MoleRaymond Christopher LimNo ratings yet
- Submitted by Manjari Reshikesh Iv Bds Part Ii Department of Oral and Maxillofacial SurgeryDocument51 pagesSubmitted by Manjari Reshikesh Iv Bds Part Ii Department of Oral and Maxillofacial SurgerykishoreNo ratings yet
- Understanding Ameloblastoma: A True Neoplasm of Enamel Organ TissueDocument51 pagesUnderstanding Ameloblastoma: A True Neoplasm of Enamel Organ TissueDrRobin SabharwalNo ratings yet
- ODONTOGENIC TUMORS LectureDocument133 pagesODONTOGENIC TUMORS LectureSama N SamirNo ratings yet
- Sarang Suresh HotchandaniDocument33 pagesSarang Suresh HotchandaniHaroon ButtNo ratings yet
- A Melo Blast OmaDocument46 pagesA Melo Blast OmaMahima SinghNo ratings yet
- 10.odontogenic TumorsDocument102 pages10.odontogenic Tumorsabdelrahman amrNo ratings yet
- Benign Odontogenic Tumou1rDocument67 pagesBenign Odontogenic Tumou1rVISHAL DHIMANNo ratings yet
- ContentDocument48 pagesContentRajat Nangia100% (1)
- Special Lecture 14Document25 pagesSpecial Lecture 14HussainNo ratings yet
- 11-Odontogenic Tumours 2Document118 pages11-Odontogenic Tumours 2Ash ArmyNo ratings yet
- Odontogenic TumorsDocument13 pagesOdontogenic Tumorsa.ahmed4922No ratings yet
- 10-ODONTOGENIC Tumours 1Document124 pages10-ODONTOGENIC Tumours 1Ash Army100% (1)
- Mixed Tumors of Odontogenic Origin WordDocument31 pagesMixed Tumors of Odontogenic Origin WordAshimNo ratings yet
- 2 - Epithelial Odontogenic TumorsDocument9 pages2 - Epithelial Odontogenic Tumorscath.rada17No ratings yet
- Department of Oral Patho Nishter Institute of Dentistry: Title 03 April 2020Document5 pagesDepartment of Oral Patho Nishter Institute of Dentistry: Title 03 April 2020umaima rizwanNo ratings yet
- Odontogenic TumoursDocument16 pagesOdontogenic TumoursSkAliHassanNo ratings yet
- Odontogenic Cysts and Tumors GuideDocument41 pagesOdontogenic Cysts and Tumors GuideSeca mandiNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- Oral Pathology - Pathology of JawsDocument35 pagesOral Pathology - Pathology of JawsamaliaNo ratings yet
- Tumors of The Jaw and Oral MucosaDocument18 pagesTumors of The Jaw and Oral MucosaDaniela LeonteNo ratings yet
- 7 - Benign Odontogenic TumorsDocument53 pages7 - Benign Odontogenic Tumorsxpxx19373No ratings yet
- Bone Tumors: Osteoma, Osteosarcoma, and MoreDocument12 pagesBone Tumors: Osteoma, Osteosarcoma, and MoreAyushi GoelNo ratings yet
- Cysts and Odontogenic Tumors4Document54 pagesCysts and Odontogenic Tumors4abolojeenNo ratings yet
- Oral Pathology Guide to Tumors and LesionsDocument41 pagesOral Pathology Guide to Tumors and LesionsAprillia Dian PertiwiNo ratings yet
- Cysts DentalDocument23 pagesCysts DentalApollo DentalNo ratings yet
- الهامDocument18 pagesالهامmoh.ahm3040No ratings yet
- A comprehensive overview of odontogenic tumors: classifications, clinical features, radiology, histopathology, treatment and prognosisDocument90 pagesA comprehensive overview of odontogenic tumors: classifications, clinical features, radiology, histopathology, treatment and prognosisNur IbrahimNo ratings yet
- Session 8 Odontogenic and Non Odontogenic TumorsDocument74 pagesSession 8 Odontogenic and Non Odontogenic TumorsZNo ratings yet
- Odontogenic Cysts: Dr. Amin AbusallamahDocument82 pagesOdontogenic Cysts: Dr. Amin Abusallamahmabula masungaNo ratings yet
- Ameloblastoma 140624025211 Phpapp02Document51 pagesAmeloblastoma 140624025211 Phpapp02agusNo ratings yet
- Radiopacitiesofjaws 160229165805 160916155535 1Document63 pagesRadiopacitiesofjaws 160229165805 160916155535 1mohamedNo ratings yet
- Odontogenic Tumor: Oral PathologyDocument17 pagesOdontogenic Tumor: Oral PathologyJoker KillerNo ratings yet
- Odontogenic Tumors and Related Jaw Lesions: A) Benign Epithelial TumorsDocument19 pagesOdontogenic Tumors and Related Jaw Lesions: A) Benign Epithelial Tumorsluna zeidNo ratings yet
- Odontogenic TumoursDocument12 pagesOdontogenic Tumoursluke swanepoelNo ratings yet
- Life Cycle of AmeloblastDocument47 pagesLife Cycle of AmeloblastdrrnonhelmyNo ratings yet
- Oral Pathology: Odontogenic TumorsDocument5 pagesOral Pathology: Odontogenic Tumorsعلي صادق جعفرNo ratings yet
- Oral Pathology: 2-Mesenchymal Origin Tumors A - Odontogenic FibromaDocument4 pagesOral Pathology: 2-Mesenchymal Origin Tumors A - Odontogenic Fibromaعلي صادق جعفرNo ratings yet
- Odonto Genic TumorsDocument7 pagesOdonto Genic TumorsMcmac YangoNo ratings yet
- cysts 1-مدمجDocument306 pagescysts 1-مدمجأمال داودNo ratings yet
- Tumor of Salivary GlandDocument28 pagesTumor of Salivary GlandrajshreeNo ratings yet
- Dr. EBTISAM ELHAMALAWY Dental AnatomyDocument65 pagesDr. EBTISAM ELHAMALAWY Dental AnatomyMustafa H. KadhimNo ratings yet
- Jaw LesionsDocument11 pagesJaw LesionsJose SirittNo ratings yet
- Cysts of The Jaws and Neck: Wil Dustin P. SinlaoDocument46 pagesCysts of The Jaws and Neck: Wil Dustin P. Sinlaojamaica faith ramonNo ratings yet
- CystDocument59 pagesCystHarshini DonepudiNo ratings yet
- CementumDocument10 pagesCementumviolaNo ratings yet
- Benign Nonodontogenic TumorsDocument20 pagesBenign Nonodontogenic TumorsEuginia YosephineNo ratings yet
- 4.benign Odontogenic and Non-Odontogenic Tumors of The Jaws - SlidesDocument45 pages4.benign Odontogenic and Non-Odontogenic Tumors of The Jaws - SlidesTarlan FarhadiNo ratings yet
- 11-Odontogenic Tumours 2Document118 pages11-Odontogenic Tumours 2Ash ArmyNo ratings yet
- Oral Pathology TumorsDocument17 pagesOral Pathology TumorsAsh ArmyNo ratings yet
- 10-ODONTOGENIC Tumours 1Document124 pages10-ODONTOGENIC Tumours 1Ash Army100% (1)
- NRSG 2445 ARDS AssignmentDocument4 pagesNRSG 2445 ARDS AssignmentregisterednurseNo ratings yet
- Polycythemia VeraDocument4 pagesPolycythemia VeraAllyson VillarNo ratings yet
- Quantitative Platelet Disorder: Hannie M. SacatanDocument24 pagesQuantitative Platelet Disorder: Hannie M. SacatanFearless AngelNo ratings yet
- ABG InterpretationDocument38 pagesABG Interpretationmahmod omerNo ratings yet
- Effects of Free Condoms On HIV and STI in MSMDocument25 pagesEffects of Free Condoms On HIV and STI in MSMHarrah Kyn GaniaNo ratings yet
- Our Sacrospinous FixationDocument3 pagesOur Sacrospinous Fixationopi setiaNo ratings yet
- Malaria 2018Document11 pagesMalaria 2018gerges8723No ratings yet
- CH4 Patho D&R AgamDocument28 pagesCH4 Patho D&R AgamS Balagopal SivaprakasamNo ratings yet
- NCP Rheumatoid Arthritis DX IpmDocument2 pagesNCP Rheumatoid Arthritis DX IpmPatty RomeroNo ratings yet
- Dyspepsia factors in Bangkinang City health center areaDocument12 pagesDyspepsia factors in Bangkinang City health center areaSofia NaimahNo ratings yet
- Benign Familial HematuriaDocument6 pagesBenign Familial Hematuriasiska_mariannaNo ratings yet
- List of Cephalosporins + Uses, Types & Side EffectsDocument5 pagesList of Cephalosporins + Uses, Types & Side EffectsMd. Sabit Ahsan SarkerNo ratings yet
- Congestive Heart Failure Case StudyDocument20 pagesCongestive Heart Failure Case StudyMegan100% (1)
- RT 255 Mammo A & P 200810Document75 pagesRT 255 Mammo A & P 200810florianqordjaNo ratings yet
- Original Article: A Clinical and Microbial Study of Otomycosis: An Original StudyDocument9 pagesOriginal Article: A Clinical and Microbial Study of Otomycosis: An Original StudywennyrhyNo ratings yet
- Medication - ALT-Template - Ferrous SulfateDocument1 pageMedication - ALT-Template - Ferrous SulfateNancyAmissahNo ratings yet
- Calcium AcetateDocument3 pagesCalcium AcetateKIM NAMJOON'S PEACHES & CREAM100% (1)
- Common Sports Injuries: August 2016Document8 pagesCommon Sports Injuries: August 2016Binte SajjadNo ratings yet
- Clinodactyly: Christian Dumontier MD, PHD Centre de La Main-Guadeloupe - FwiDocument34 pagesClinodactyly: Christian Dumontier MD, PHD Centre de La Main-Guadeloupe - FwiProfesseur Christian Dumontier0% (1)