You might also like
- Differently Able: Embracing Diversity in Disabilities A Journey Through Acceptance, Empowerment, and InclusionFrom EverandDifferently Able: Embracing Diversity in Disabilities A Journey Through Acceptance, Empowerment, and InclusionNo ratings yet
- Inclusiveness (Chapter 1 & 2)Document71 pagesInclusiveness (Chapter 1 & 2)ffff100% (1)
- "We Care For You": Sensitizing Youth Towards Differently AbledDocument13 pages"We Care For You": Sensitizing Youth Towards Differently AbledNamrata GuptaNo ratings yet
- Daraaraa Thesis 1Document3 pagesDaraaraa Thesis 1Guutaa DirbabaaNo ratings yet
- The Right of Persons With Disabilities To Live in The CommunityDocument35 pagesThe Right of Persons With Disabilities To Live in The CommunityIipo ChennaiNo ratings yet
- DISABILITY 101 LatestDocument27 pagesDISABILITY 101 LatestNachyAloysiusNo ratings yet
- The Social Assistance For People With DisabilitiesDocument5 pagesThe Social Assistance For People With DisabilitiessunshineakhanovaNo ratings yet
- Why Disability Matters: Suzanne C. Smeltzer, Edd, RN, Anef, FaanDocument23 pagesWhy Disability Matters: Suzanne C. Smeltzer, Edd, RN, Anef, FaanMichaelMinhNgoNo ratings yet
- CBR Committee Establishment TrainingDocument26 pagesCBR Committee Establishment Trainingsiyoum negashNo ratings yet
- Impairment and Disability-1Document22 pagesImpairment and Disability-1Regina PunNo ratings yet
- PSB Introduction To DisabilityDocument26 pagesPSB Introduction To Disabilityapi-261503220100% (2)
- 1.2 MalaysiaDocument46 pages1.2 MalaysiaslpheyNo ratings yet
- Disability in SomaliaDocument22 pagesDisability in SomaliaSamira HassanNo ratings yet
- World Report On Disability FactsheetDocument2 pagesWorld Report On Disability Factsheetkismatadhikari141No ratings yet
- Helpage International: Our Vision: Is A World in Which All Older PeopleDocument34 pagesHelpage International: Our Vision: Is A World in Which All Older PeopleMujeeb RehmanNo ratings yet
- Persons With DisabilityDocument42 pagesPersons With DisabilityJuvy IringanNo ratings yet
- Impact of Disability and Vulnerability On Daily Life: Learning OutcomesDocument52 pagesImpact of Disability and Vulnerability On Daily Life: Learning OutcomesAsnake Yohanis80% (5)
- UNDERSTANDING GENDER EQUALITY, DISABILITY by Humanitarian GlobalDocument49 pagesUNDERSTANDING GENDER EQUALITY, DISABILITY by Humanitarian Globalabdella abduNo ratings yet
- Role of Public Health in Addressing Physical DisabilitiesDocument12 pagesRole of Public Health in Addressing Physical DisabilitiesAli RazaNo ratings yet
- Ch. 19 DisabilitiesDocument16 pagesCh. 19 DisabilitiesJenn StyronNo ratings yet
- Special Needs Education, PPT 1, 2 & 3 Combined-1Document132 pagesSpecial Needs Education, PPT 1, 2 & 3 Combined-1wongani phiri100% (1)
- Disability DataDocument45 pagesDisability DataAuberon Jeleel OdoomNo ratings yet
- EnglishDocument22 pagesEnglishanshicaNo ratings yet
- Legal Issues Regarding HandicappedDocument28 pagesLegal Issues Regarding HandicappedBina AgrahariNo ratings yet
- Chapter 3 FINAL Identification of The Impact of Disability & DifferentiatedDocument52 pagesChapter 3 FINAL Identification of The Impact of Disability & DifferentiatedHunde AdamuNo ratings yet
- Universal Design 1Document10 pagesUniversal Design 1VipulNo ratings yet
- Unit-Ii Psychology of DisabilityDocument24 pagesUnit-Ii Psychology of DisabilityShubhashri AcharyaNo ratings yet
- What Is The Role of Medical Services On The Implementation of Different Interventions For People With Disabilities?Document2 pagesWhat Is The Role of Medical Services On The Implementation of Different Interventions For People With Disabilities?Õbsëqúiœus Menam MikreNo ratings yet
- Module1 WhatDisabilityDocument21 pagesModule1 WhatDisabilityAnithamol BabuNo ratings yet
- Groups in Context: DisabilitiesDocument10 pagesGroups in Context: Disabilitiesapi-409521281No ratings yet
- Social Work Disability Rights in Pakistan: Submitted To: Ma'am Rizwana. Submitted By: Sidra ShahbazDocument8 pagesSocial Work Disability Rights in Pakistan: Submitted To: Ma'am Rizwana. Submitted By: Sidra ShahbazAhmedHassanKanjuNo ratings yet
- Chapter 3 InclusivenessDocument30 pagesChapter 3 InclusivenessAbuzakir IdirisNo ratings yet
- Relevance of Disability Models From The Perspective of A Developing CountryDocument13 pagesRelevance of Disability Models From The Perspective of A Developing CountryAlexander Decker100% (2)
- Research Final Submission 21.07.18Document38 pagesResearch Final Submission 21.07.18Ian Kristopher BayanNo ratings yet
- A New Vision of Funding - A NewDocument14 pagesA New Vision of Funding - A NewFiona Kumari CampbellNo ratings yet
- Impairment, Disability and RehabilitationsDocument29 pagesImpairment, Disability and RehabilitationsEric AmacksonNo ratings yet
- CHAPTER TWO InclsnDocument18 pagesCHAPTER TWO InclsnezakbelachewNo ratings yet
- Chapter 3 - Identifications of Impacts of DisabilityDocument39 pagesChapter 3 - Identifications of Impacts of Disabilityshelema lemiNo ratings yet
- Inclusiveness in Natural ScienceDocument157 pagesInclusiveness in Natural ScienceJOKER MulualemNo ratings yet
- Differently AbledDocument16 pagesDifferently AbledAditi Gaur100% (1)
- Inclusivness AssignmentDocument17 pagesInclusivness AssignmentEphrem ChernetNo ratings yet
- Provide Appropriate Support To People With Special NeedsDocument39 pagesProvide Appropriate Support To People With Special NeedsKass Pangilinan88% (8)
- Disability YyDocument4 pagesDisability Yyvishal23713284No ratings yet
- Social Inclusion of Persons With DisabilitiesDocument24 pagesSocial Inclusion of Persons With DisabilitiesCassey Reign MendozaNo ratings yet
- Group 5Document24 pagesGroup 5Clarisse RamosNo ratings yet
- LMIR Issue No. 1, S. 2020 - Enabling The DisabledDocument34 pagesLMIR Issue No. 1, S. 2020 - Enabling The DisabledMarigold CherieNo ratings yet
- Differently AbledDocument14 pagesDifferently AbledRidhi Goel100% (1)
- Inclusive Chapter ThreeDocument21 pagesInclusive Chapter ThreeAbazer SultanNo ratings yet
- Inclusiveness: Addis Ababa University College of Education and Behavioral Studies Department of Special Needs EducationDocument49 pagesInclusiveness: Addis Ababa University College of Education and Behavioral Studies Department of Special Needs EducationĒrmias Álemayehu100% (2)
- Disability Inclusion: About This GuidanceDocument4 pagesDisability Inclusion: About This GuidanceAlexander MartinezNo ratings yet
- EVALUATION 8 February 3 - FCM 3Document11 pagesEVALUATION 8 February 3 - FCM 3Maureen Via Madrid ComiaNo ratings yet
- Universal Accessibility of Nehru PlaceDocument40 pagesUniversal Accessibility of Nehru PlaceGautam kumarNo ratings yet
- Understanding Disabilitypdf PDFDocument17 pagesUnderstanding Disabilitypdf PDFArnold ArubaNo ratings yet
- Chapter 3Document49 pagesChapter 3Melaku Walelgne100% (1)
- Group No.-5 Issues of People With Physical DisabilityDocument21 pagesGroup No.-5 Issues of People With Physical Disabilityharsh gawliNo ratings yet
- Week 10 Vulnerable PopulationsDocument44 pagesWeek 10 Vulnerable PopulationsMohd ArifNo ratings yet
- APG Team Nila Courts 1 Disability AwarenessDocument44 pagesAPG Team Nila Courts 1 Disability AwarenessJingyi SaysHelloNo ratings yet
- Models of Disability Lecture 2021Document23 pagesModels of Disability Lecture 2021Danielle GrguricNo ratings yet
- OLD Mutual AssignmentDocument15 pagesOLD Mutual AssignmentashNo ratings yet
- Disability Awareness and Inclusion Training (RDM Hawassa)Document45 pagesDisability Awareness and Inclusion Training (RDM Hawassa)Moti BatuNo ratings yet
- Antimicrobial Spectrum and Characteristics of Hand-Hygiene Antiseptic AgentsDocument3 pagesAntimicrobial Spectrum and Characteristics of Hand-Hygiene Antiseptic AgentsdonsterthemonsterNo ratings yet
- Animal ExtinctionDocument2 pagesAnimal Extinctionaliah hudaNo ratings yet
- Lab 9Document3 pagesLab 9Tâm NguyễnNo ratings yet
- Midview of 2Document4 pagesMidview of 2api-285760777No ratings yet
- Chapter 6 MotivationDocument39 pagesChapter 6 MotivationyurmumgayNo ratings yet
- Sustainable Transportation and Electric VehiclesDocument17 pagesSustainable Transportation and Electric Vehicless131744No ratings yet
- Product Selector Guide Marine Protective Coatings en 196830Document1 pageProduct Selector Guide Marine Protective Coatings en 196830wilberizquierdo1No ratings yet
- Abstract Yessy Marzona Icge VDocument21 pagesAbstract Yessy Marzona Icge VYessy MarzonaNo ratings yet
- Solution Methods For Nonlinear Finite Element Analysis (NFEA)Document39 pagesSolution Methods For Nonlinear Finite Element Analysis (NFEA)janaaidaas1996No ratings yet
- Lesson Plan Ordinal NumbersDocument5 pagesLesson Plan Ordinal Numbersapi-329663096No ratings yet
- Solar Brochure February 2023Document24 pagesSolar Brochure February 2023prakistaoNo ratings yet
- A Level NdebeleDocument5 pagesA Level Ndebelenokwandadlamini2010No ratings yet
- Basic Electronics New - 3110016Document4 pagesBasic Electronics New - 3110016Sneha PandyaNo ratings yet
- NewJaisa Corporate ProfileDocument14 pagesNewJaisa Corporate ProfileCRAZY ಕನ್ನಡಿಗNo ratings yet
- List of Homoeopathic Medicines, Combinations & Their UsesDocument29 pagesList of Homoeopathic Medicines, Combinations & Their Usesgirish261187% (55)
- UntitledDocument42 pagesUntitledDiana JacquelineNo ratings yet
- Abs TechnologyDocument14 pagesAbs Technologyanime landNo ratings yet
- Imanager U2000 ME Release Notes 01 PDFDocument180 pagesImanager U2000 ME Release Notes 01 PDFCamilo Andres OrozcoNo ratings yet
- TSX Datasheet 2021 05Document10 pagesTSX Datasheet 2021 05Filipe LaínsNo ratings yet
- Gelatin Film Lysis TestDocument2 pagesGelatin Film Lysis TestSuryakant HayatnagarkarNo ratings yet
- WASA Wastewater and Potable Water Design Requirements PDFDocument233 pagesWASA Wastewater and Potable Water Design Requirements PDFYassin AlkadyNo ratings yet
- HSE Manager JDDocument2 pagesHSE Manager JDRukun SinagaNo ratings yet
- D.ANDAN PS-PROJECT WATCH ActionPlan 2018-2019Document3 pagesD.ANDAN PS-PROJECT WATCH ActionPlan 2018-2019Maria Fe PanuganNo ratings yet
- 6 Pre-Transfusion TestingDocument24 pages6 Pre-Transfusion TestingRhema AyuhNo ratings yet
- Candidate Guide SCR24Document16 pagesCandidate Guide SCR24Michael JunusNo ratings yet
- Beamray 50R100R Data SheetDocument2 pagesBeamray 50R100R Data Sheethassan elgamriNo ratings yet
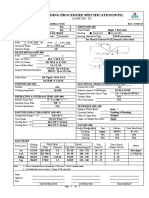
- Welding Procedure Specification (WPS) : (Asme Sec. Ix)Document1 pageWelding Procedure Specification (WPS) : (Asme Sec. Ix)Ahmed Lepda100% (1)
- Research: A Review and A PreviewDocument79 pagesResearch: A Review and A PreviewJonathan SiguinNo ratings yet
- Assignment On I.T & Pharma IndustryDocument11 pagesAssignment On I.T & Pharma IndustryGolu SinghNo ratings yet
- FC52Document5 pagesFC52Bassel AlmouieNo ratings yet