You might also like
- SympathomimeticDocument56 pagesSympathomimeticvarish0% (1)
- INOTROPESDocument28 pagesINOTROPESsinghal297% (30)
- Adrenergic AgentsDocument45 pagesAdrenergic AgentsAmit ShahNo ratings yet
- Adrenergic Drugs: Pharmacological Department Medical School - UNPAD Ike HusenDocument33 pagesAdrenergic Drugs: Pharmacological Department Medical School - UNPAD Ike HusenHendra EfendiNo ratings yet
- CHFDocument11 pagesCHFGwendolyn Talahiban LusaraNo ratings yet
- Sympathomimetics (Catecholamines & Non Catecholamines)Document99 pagesSympathomimetics (Catecholamines & Non Catecholamines)Raheel JavaidNo ratings yet
- 2 Adrenergic SystemDocument14 pages2 Adrenergic SystemAli EllaffiNo ratings yet
- Pharmacology of Adrenergic AgonistsDocument9 pagesPharmacology of Adrenergic Agonistsfiena92No ratings yet
- Adrenergic AgonistsDocument52 pagesAdrenergic AgonistsTsegaye HailuNo ratings yet
- Adrenergic DrugsDocument14 pagesAdrenergic DrugsMarian YuqueNo ratings yet
- Sympathomimetics Physical Therapy NewDocument25 pagesSympathomimetics Physical Therapy NewMohamed MoustafaNo ratings yet
- YogeshDocument49 pagesYogeshapi-3741769No ratings yet
- Adrenergic ReceptorsDocument7 pagesAdrenergic Receptorsaiesha.khalid.1980No ratings yet
- Pharmacology Notes: By: Khurram AbbasDocument48 pagesPharmacology Notes: By: Khurram AbbasAsma AnjumNo ratings yet
- Adrenergic DrugsDocument50 pagesAdrenergic DrugscoleenNo ratings yet
- Adrenergic Drugs 20.06.018 PDFDocument55 pagesAdrenergic Drugs 20.06.018 PDFHitesh karnNo ratings yet
- Adrenoceptor Agonist and Antagonist Drugs-2014.10.7pptDocument83 pagesAdrenoceptor Agonist and Antagonist Drugs-2014.10.7pptking_gold100% (1)
- Sympathomimetic - AdrenergicDocument3 pagesSympathomimetic - AdrenergicRohit GodaseNo ratings yet
- 05-Adrenergic Agonists DR Hala 2020Document30 pages05-Adrenergic Agonists DR Hala 2020مشاعرمبعثرةNo ratings yet
- AdrenomimimeticsDocument40 pagesAdrenomimimeticshealer sruthyNo ratings yet
- Pharmacology NotesDocument48 pagesPharmacology NotesBheru Lal100% (1)
- Inotropes and VasopressorsDocument63 pagesInotropes and VasopressorsCraig DuHaney50% (2)
- Autonomic Nervous System AgentsDocument120 pagesAutonomic Nervous System Agentscoosa liquors100% (1)
- Adrenergic AgentsDocument69 pagesAdrenergic Agents4pm6gjq78cNo ratings yet
- Adrenergic AntagonistDocument30 pagesAdrenergic AntagonistOmar AlaamNo ratings yet
- Adrenergic Receptors and DrugsDocument67 pagesAdrenergic Receptors and DrugsNaghman Zuberi100% (2)
- PharmTest3 StudyGuideDocument9 pagesPharmTest3 StudyGuideTara Bickford ManisNo ratings yet
- Adrenaline & Noradrenaline: DR Nida Fatima Jawaharlal Nehru Medical College, Amu AligarhDocument46 pagesAdrenaline & Noradrenaline: DR Nida Fatima Jawaharlal Nehru Medical College, Amu AligarhDivya Rekha KolliNo ratings yet
- Adrenergic DrugsDocument45 pagesAdrenergic DrugsHUZAIFA YAMAANNo ratings yet
- Adrenergic Drugs 20.07.018 PDFDocument59 pagesAdrenergic Drugs 20.07.018 PDFHitesh karnNo ratings yet
- Autonomic Nervous System AgentsDocument14 pagesAutonomic Nervous System AgentsRhenier S. Ilado100% (1)
- Pharma FlashcardsDocument14 pagesPharma Flashcardszm_khalidNo ratings yet
- By: Professor Emiliano Z. Sison JRDocument40 pagesBy: Professor Emiliano Z. Sison JRT Z BenNo ratings yet
- ANS2Document16 pagesANS2yaya mohaNo ratings yet
- PHARMACOLOGY (Autocoid-Renal-GI-CV-CNS)Document33 pagesPHARMACOLOGY (Autocoid-Renal-GI-CV-CNS)Famela Anne GOmez MadambaNo ratings yet
- FARMAKOLOGI OBAT VASOPRESOR-dr DjujukDocument25 pagesFARMAKOLOGI OBAT VASOPRESOR-dr DjujukjavajavuNo ratings yet
- Farmakologi Obat VasopresorDocument25 pagesFarmakologi Obat Vasopresorhendrik taufikNo ratings yet
- Farmakologi Obat VasopresorDocument25 pagesFarmakologi Obat VasopresorNudyan BetharinaNo ratings yet
- Pharmacology - Section 07 - Inotropes and PressorsDocument6 pagesPharmacology - Section 07 - Inotropes and PressorsPathalee ThalpavilaNo ratings yet
- Sympathomimetic Drugs: Dr. Shazana RanaDocument78 pagesSympathomimetic Drugs: Dr. Shazana Ranaمحمد رافع تنویر100% (1)
- Helping Material For PrometricDocument48 pagesHelping Material For PrometricRPh FarhatainNo ratings yet
- Exam 1 Pharmacology II NotesDocument4 pagesExam 1 Pharmacology II Notessin2begin2No ratings yet
- Lecture 6 - Adrenergic AgonistsDocument24 pagesLecture 6 - Adrenergic AgonistsHadiya RohitNo ratings yet
- Adrenergic SystemDocument6 pagesAdrenergic SystemdocsNo ratings yet
- Antihypertensive AgentsDocument41 pagesAntihypertensive AgentsRwapembe StephenNo ratings yet
- Assignment On Adrenergic ReceptorDocument13 pagesAssignment On Adrenergic ReceptoryannaingNo ratings yet
- Obat SimpatomimetikDocument42 pagesObat SimpatomimetiknatinlalaNo ratings yet
- Adrenergic AntagonistsDocument6 pagesAdrenergic Antagonistsfiena92100% (2)
- SympathomimeticDocument71 pagesSympathomimeticahmad tariqNo ratings yet
- SympatheticDocument10 pagesSympatheticSharneeshriyaNo ratings yet
- PharmacologyDocument46 pagesPharmacologyvinupv88No ratings yet
- L18 - Adrenergics IIIDocument10 pagesL18 - Adrenergics IIIyasaira707No ratings yet
- Drenergic AND Anti Adrenergic Drugs: Shabib AkhtarDocument21 pagesDrenergic AND Anti Adrenergic Drugs: Shabib AkhtarDeepa ShaiekhNo ratings yet
- Drugs For Treating Heart FailureDocument40 pagesDrugs For Treating Heart FailureMbah GapinbissiNo ratings yet
- Physiological Review For CV DrugsDocument21 pagesPhysiological Review For CV DrugsatinafansifNo ratings yet
- 9 Drugs Affecting Angina PectorisDocument3 pages9 Drugs Affecting Angina PectoristiaraNo ratings yet
- Pharmacology of Inotropes and VasopressorsDocument51 pagesPharmacology of Inotropes and VasopressorsApen Silaban100% (1)
- Adrenergic DrugsDocument58 pagesAdrenergic DrugsMuzammil Nawaz100% (1)
- 03 - Pharmacology of Drugs Affecting Adrenergic Synapses.Document62 pages03 - Pharmacology of Drugs Affecting Adrenergic Synapses.ashishanandaakNo ratings yet
- Routes of Drug Administration and Dosage FormsDocument39 pagesRoutes of Drug Administration and Dosage FormsAditya RathoreNo ratings yet
- General PharmacologyDocument101 pagesGeneral PharmacologyAditya RathoreNo ratings yet
- Chemistry Investigatory Project 2018-19: Setting of CementDocument18 pagesChemistry Investigatory Project 2018-19: Setting of CementNitin Sai AvirneniNo ratings yet
- CHEMISTRY (Code No. 043) 2019-20: RationaleDocument26 pagesCHEMISTRY (Code No. 043) 2019-20: RationaleShivamNo ratings yet
- FileHandler PDFDocument1 pageFileHandler PDFAditya RathoreNo ratings yet
- CHEMISTRY (Code No. 043) 2019-20: RationaleDocument26 pagesCHEMISTRY (Code No. 043) 2019-20: RationaleShivamNo ratings yet
- Human Medicines Highlights March 2023 - enDocument9 pagesHuman Medicines Highlights March 2023 - enrodcam1No ratings yet
- E C T Document PDFDocument17 pagesE C T Document PDFDhAiRyA ArOrANo ratings yet
- Transient Tachypnea of The NewbornDocument53 pagesTransient Tachypnea of The NewbornAyah PaasaNo ratings yet
- Mefenamic Acid Drug StudyDocument1 pageMefenamic Acid Drug StudyBer AnneNo ratings yet
- Omsite 2005 PDFDocument180 pagesOmsite 2005 PDFJulie100% (2)
- Psyche ReviewerDocument13 pagesPsyche ReviewerKem100% (1)
- RENAL QuestionDocument15 pagesRENAL QuestionAnne CortezNo ratings yet
- Ampicillin SulbactamDocument3 pagesAmpicillin Sulbactamrhon_123rd88% (17)
- DRUG STUDY FINAL (Onco) PDFDocument14 pagesDRUG STUDY FINAL (Onco) PDFFrancis Anthony LoslosoNo ratings yet
- Does This Patient Have Clubbing PDFDocument7 pagesDoes This Patient Have Clubbing PDFAhraxazel Galicia ReynaNo ratings yet
- Lipid Profile Disease and DiagnosisDocument31 pagesLipid Profile Disease and DiagnosisGeetanjali Jha100% (1)
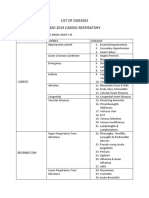
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- Human Genetic Disorders: Photos Are From Smith's Recognizable Patterns of HumanDocument49 pagesHuman Genetic Disorders: Photos Are From Smith's Recognizable Patterns of HumanJessie AzarragaNo ratings yet
- Hepatic SteatosisDocument9 pagesHepatic Steatosiss12144017No ratings yet
- Autoimmune - Hemolytic - Anemia - Mixed - Type-A - Case - Repo 2Document5 pagesAutoimmune - Hemolytic - Anemia - Mixed - Type-A - Case - Repo 2Afsha AnishNo ratings yet
- Hema Chapter 21 Part 2Document4 pagesHema Chapter 21 Part 2EMETERIO TUTOR IIINo ratings yet
- Doña Remedios Trinidad Romualdez Medical Foundation Inc. College of Medicine Calanipawan Road, Tacloban City, LeyteDocument2 pagesDoña Remedios Trinidad Romualdez Medical Foundation Inc. College of Medicine Calanipawan Road, Tacloban City, LeyteIrish AlonzoNo ratings yet
- Siegelman Online Advantage 1.1 PDFDocument39 pagesSiegelman Online Advantage 1.1 PDFDana Ysabelle Ibarra100% (1)
- Krok 2 2002-2003 TherapyDocument41 pagesKrok 2 2002-2003 TherapyAli ZeeshanNo ratings yet
- Harrison - S Principles of Internal Medicine - Self PDFDocument27 pagesHarrison - S Principles of Internal Medicine - Self PDFSydrex Sarmiento0% (1)
- Eye Docs General MedicineDocument125 pagesEye Docs General MedicineMuneeb ShahzadNo ratings yet
- Journal OsteochondromaDocument14 pagesJournal OsteochondromaAnggi CalapiNo ratings yet
- Treatment of Post-Traumatic Hematoma and Fibrosis Using Hyaluronidase 2019Document4 pagesTreatment of Post-Traumatic Hematoma and Fibrosis Using Hyaluronidase 2019maat1No ratings yet
- Nejmoa2030183 AppendixDocument34 pagesNejmoa2030183 AppendixAmna ElayanNo ratings yet
- Classification of Epilepsie1981 - ILAEDocument13 pagesClassification of Epilepsie1981 - ILAEarmythunderNo ratings yet
- NCLEX Questions For Test 3 All ChaptersDocument7 pagesNCLEX Questions For Test 3 All Chaptersctramel001No ratings yet
- Neuromuscular Junction Blocking AgentsDocument9 pagesNeuromuscular Junction Blocking AgentsSyvNo ratings yet
- Porphyria: By: Sheena Joy Barredo Mls 3DDocument31 pagesPorphyria: By: Sheena Joy Barredo Mls 3DEdgar DumagpiNo ratings yet
- ABIM Laboratory Test Reference Ranges January 2020Document12 pagesABIM Laboratory Test Reference Ranges January 2020jaumeNo ratings yet
- ДД округлых образований (методичка)Document15 pagesДД округлых образований (методичка)Sriram Lakshmanan LNo ratings yet