You might also like
- Myasthenia Gravis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMyasthenia Gravis, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Neurologicdisorders 100816033614 Phpapp01 PDFDocument96 pagesNeurologicdisorders 100816033614 Phpapp01 PDFenam professorNo ratings yet
- Multiple SclerosisDocument3 pagesMultiple Sclerosisapi-3822433No ratings yet
- Guillain Barre Syndrome-PPT FinalDocument39 pagesGuillain Barre Syndrome-PPT Finalmeghana100% (1)
- Diabetic Neuropathy: DR Shahjada SelimDocument129 pagesDiabetic Neuropathy: DR Shahjada SelimmadboyNo ratings yet
- Add A Slide Title - 1Document23 pagesAdd A Slide Title - 1Salman SalmanNo ratings yet
- Neurological Stressors III Chronic Neurological Disorders: Joy Borrero, RN, MSN and NUR240 Nursing StudentsDocument38 pagesNeurological Stressors III Chronic Neurological Disorders: Joy Borrero, RN, MSN and NUR240 Nursing StudentsCristina CenturionNo ratings yet
- Multiple SclerosisDocument46 pagesMultiple SclerosisMadeline Jessica HuwaeNo ratings yet
- Multiple SclerosisDocument19 pagesMultiple Sclerosis27b7976xtjNo ratings yet
- Multiple SclerosisDocument34 pagesMultiple SclerosisDe Sesto Rhys Carlo0% (1)
- Geriatric DisorderDocument49 pagesGeriatric Disordersidd7rNo ratings yet
- Management of Patient With Meningitis and Encephalitis: ModeratorDocument71 pagesManagement of Patient With Meningitis and Encephalitis: ModeratorSachin DwivediNo ratings yet
- Neuro DisordersDocument60 pagesNeuro DisordersLovelights ZamoraNo ratings yet
- Endocrine DisordersDocument54 pagesEndocrine Disorderspradeep pintoNo ratings yet
- Movement Disorder in ChildrenDocument35 pagesMovement Disorder in Childrenstandar 1 neuroNo ratings yet
- Guillain Barre SyndromeDocument32 pagesGuillain Barre SyndromeDada MundaNo ratings yet
- Guillain-Barré Syndrome: Presented byDocument31 pagesGuillain-Barré Syndrome: Presented bySanjay SilwalNo ratings yet
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocument96 pagesN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaNo ratings yet
- Dizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineDocument34 pagesDizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineManish Chandra PrabhakarNo ratings yet
- CP 11 MX of Spinal Cord DisordersDocument44 pagesCP 11 MX of Spinal Cord DisordersNur Amaleeza Abdul MananNo ratings yet
- EpilepsyDocument73 pagesEpilepsyabenezer g/kirstosNo ratings yet
- Case Presentation - GBSDocument28 pagesCase Presentation - GBSJan Marvin Lichauco MendozaNo ratings yet
- Peripheral Nerve and Muscular WeaknessDocument17 pagesPeripheral Nerve and Muscular WeaknessSamuel kuriaNo ratings yet
- Guillain Barre Syndrome (GBS)Document29 pagesGuillain Barre Syndrome (GBS)Sujit KoiralaNo ratings yet
- Myasthenia Gravis: DR Aung Paing Phyo PG3 AnesthesiaDocument72 pagesMyasthenia Gravis: DR Aung Paing Phyo PG3 AnesthesiaAg Paing PhyoNo ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadisradiologi igdNo ratings yet
- List of Problems The Patient HasDocument5 pagesList of Problems The Patient HasKiruba SelvamNo ratings yet
- Guillian Baare Syndrome: Mr. Jeo Thomas 1 M.SC Nursing SconDocument38 pagesGuillian Baare Syndrome: Mr. Jeo Thomas 1 M.SC Nursing SconJeo Thomas100% (1)
- Ageing SeminarDocument56 pagesAgeing SeminarShubham gaurNo ratings yet
- Delirium: DR A.Vijaya Chandra Reddy Associate Professor of Psychaitry Dept. of Psychiatry Rims, KadapaDocument20 pagesDelirium: DR A.Vijaya Chandra Reddy Associate Professor of Psychaitry Dept. of Psychiatry Rims, KadapaPraveen Pravii100% (1)
- Organic Mental DisorderDocument40 pagesOrganic Mental DisorderSumam NeveenNo ratings yet
- Myasthenia GravisDocument30 pagesMyasthenia GravisMridula Mary AugustineNo ratings yet
- Multiple Sclerosis StudentDocument9 pagesMultiple Sclerosis StudentKelly WaskoNo ratings yet
- Demyelinating DiseaseDocument42 pagesDemyelinating Diseasemirabel IvanaliNo ratings yet
- Degenerative Neurologic DisordersDocument29 pagesDegenerative Neurologic DisordersVIDYANo ratings yet
- Guillain Barre SyndromeDocument16 pagesGuillain Barre SyndromeAgnes NesiaNo ratings yet
- Guillain-Barre Syndrome: Raquel Benhayoun Amaya Rodriguez Yohanna VazquezDocument11 pagesGuillain-Barre Syndrome: Raquel Benhayoun Amaya Rodriguez Yohanna Vazquezanon_914487171No ratings yet
- Presentation Guillian Barre SyndromeDocument12 pagesPresentation Guillian Barre SyndromeKristian Karl Bautista Kiw-isNo ratings yet
- Myasthenia GravisDocument2 pagesMyasthenia GravisMarissa AsimNo ratings yet
- Neurologic DiseasesDocument13 pagesNeurologic DiseasesCzarinah BacuadoNo ratings yet
- Case 1Document12 pagesCase 1Denisa-Alexandra MănăstireanuNo ratings yet
- UNIT 5 Manage Physiol Psych Disorders - PptatypicalDocument57 pagesUNIT 5 Manage Physiol Psych Disorders - PptatypicalNicoleNo ratings yet
- Aches and Pains in The ElderlyDocument34 pagesAches and Pains in The ElderlyAna CampeanuNo ratings yet
- 005 - Polyneuropathy GBSDocument54 pages005 - Polyneuropathy GBSLucas Victor AlmeidaNo ratings yet
- Transverse MyelitisDocument16 pagesTransverse MyelitisIsolani159No ratings yet
- Diabetes: Diagnose - Fasting Plasma Glucose (FPG) - A1C Test - Random Plasma Glucose (RPG)Document9 pagesDiabetes: Diagnose - Fasting Plasma Glucose (FPG) - A1C Test - Random Plasma Glucose (RPG)ValentinaIndahFitrianiNo ratings yet
- 08.01.24 Dr. Helal, DMD, CPD-2Document60 pages08.01.24 Dr. Helal, DMD, CPD-2Minhajul IslamNo ratings yet
- Enteral Nutrition in Neurological DiseasesDocument51 pagesEnteral Nutrition in Neurological DiseasesAnonymous DA8iQzNo ratings yet
- Spine Disease and Fractures For StudentsDocument79 pagesSpine Disease and Fractures For StudentsAbdullah MohdNo ratings yet
- Fatigue: Done By: Nancy Ghishan Amr LahlouhDocument24 pagesFatigue: Done By: Nancy Ghishan Amr LahlouhazmimustafaNo ratings yet
- Brain TumorDocument50 pagesBrain TumorbudiNo ratings yet
- Myasthenia - Gravis - 4th Yr PresentationDocument32 pagesMyasthenia - Gravis - 4th Yr PresentationMalueth AnguiNo ratings yet
- Multiple SclerosisDocument30 pagesMultiple Sclerosischikanyamichelle31No ratings yet
- Organic Brain DisorderDocument69 pagesOrganic Brain DisorderHowell Mathew100% (1)
- Organic Brain Disorder-1Document69 pagesOrganic Brain Disorder-1Howell MathewNo ratings yet
- Epilepsy in Adults A Basic IntroductionDocument40 pagesEpilepsy in Adults A Basic IntroductionDrGasnasNo ratings yet
- Myasthenia GravisDocument44 pagesMyasthenia GravisAli KhaqaanNo ratings yet
- Behavioral Disorder by Dr. Mohammed AlneamiDocument49 pagesBehavioral Disorder by Dr. Mohammed AlneamimaithamNo ratings yet
- Prevention Practice For Neuromuscular Conditions PresentationDocument22 pagesPrevention Practice For Neuromuscular Conditions PresentationShimmering MoonNo ratings yet
- Heartfailurepptsam 170511135108Document48 pagesHeartfailurepptsam 170511135108enam professorNo ratings yet
- Descriptive Statistics Inferential Statistics: Chinna ChadayanDocument40 pagesDescriptive Statistics Inferential Statistics: Chinna Chadayanenam professorNo ratings yet
- Final Report Palliative Care Community Learning ProjectDocument49 pagesFinal Report Palliative Care Community Learning Projectenam professorNo ratings yet
- Palliative Care Workbook For CarersDocument100 pagesPalliative Care Workbook For Carersenam professorNo ratings yet
- Measuresofcentraltendency 230830081030 98b4dc1cDocument64 pagesMeasuresofcentraltendency 230830081030 98b4dc1cD. Melba S.S ChinnaNo ratings yet
- Bookshelf - NBK195248, Palliative CareDocument50 pagesBookshelf - NBK195248, Palliative CarefreddymataNo ratings yet
- Curriculum For Master of Science (Medical Surgical Nursing) : MGM Institute of Health SciencesDocument266 pagesCurriculum For Master of Science (Medical Surgical Nursing) : MGM Institute of Health Sciencesenam professorNo ratings yet
- Journal Club Evaluation FormDocument1 pageJournal Club Evaluation Formenam professorNo ratings yet
- Information Brochure: Nurse Practitioner in Critical Care (NPCC) (2 Years)Document17 pagesInformation Brochure: Nurse Practitioner in Critical Care (NPCC) (2 Years)enam professorNo ratings yet
- SRM Ist SRM College of Nursing M.Sc. NursingDocument145 pagesSRM Ist SRM College of Nursing M.Sc. Nursingenam professorNo ratings yet
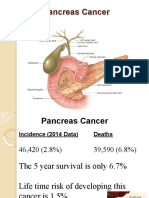
- Pancreaticcancer 150917114601 Lva1 App6891Document30 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- Research ProblemDocument13 pagesResearch ProblemKiran ThomasNo ratings yet
- Dermatitisslide 200715172028Document45 pagesDermatitisslide 200715172028enam professorNo ratings yet
- Pancreaticcancer 150917114601 Lva1 App6891Document25 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- Osteoporosis20 02 2016 160620141900 PDFDocument20 pagesOsteoporosis20 02 2016 160620141900 PDFenam professorNo ratings yet
- Dermatitisandeczema 170428113515Document12 pagesDermatitisandeczema 170428113515enam professorNo ratings yet
- Hepaticfailure 191217094905Document39 pagesHepaticfailure 191217094905enam professorNo ratings yet
- Healthindicator1 180101054753Document33 pagesHealthindicator1 180101054753enam professorNo ratings yet
- Theoretical Framework in NursingDocument27 pagesTheoretical Framework in Nursingenam professorNo ratings yet
- Pancreatitispptnitinm1st 181229090413Document58 pagesPancreatitispptnitinm1st 181229090413enam professorNo ratings yet
- Pancreascancer 140820083912 Phpapp01Document55 pagesPancreascancer 140820083912 Phpapp01enam professorNo ratings yet
- Pancreatitispptnitinm1st 181229090413Document58 pagesPancreatitispptnitinm1st 181229090413enam professorNo ratings yet
- Osteoporosis20 02 2016 160620141900Document20 pagesOsteoporosis20 02 2016 160620141900enam professorNo ratings yet
- Dorthye 210422143919Document53 pagesDorthye 210422143919enam professorNo ratings yet
- A Study To Assess The Effectiveness of Simulation Based Learning Programme On Hands-2Document29 pagesA Study To Assess The Effectiveness of Simulation Based Learning Programme On Hands-2enam professorNo ratings yet
- Female Reproductive SystemDocument69 pagesFemale Reproductive Systemenam professorNo ratings yet
- Factors Influensing Growth and DevpDocument39 pagesFactors Influensing Growth and Devpenam professorNo ratings yet
- Elderly 170825043248Document46 pagesElderly 170825043248enam professorNo ratings yet
- Advanced Steel Structure Concepts: 2 MonthsDocument4 pagesAdvanced Steel Structure Concepts: 2 MonthsAnkit SoniNo ratings yet
- PalmistryDocument116 pagesPalmistrymarinoyogaNo ratings yet
- Adminstration of Intramusclar InjectionDocument3 pagesAdminstration of Intramusclar InjectionDenise CastroNo ratings yet
- Kiss Forex How To Trade Ichimoku PDFDocument72 pagesKiss Forex How To Trade Ichimoku PDFSastryassociates Chartered100% (3)
- Phineas Gage: From The Passage of An Iron Rod Through The Head"Document1 pagePhineas Gage: From The Passage of An Iron Rod Through The Head"GlupiaSprawaNo ratings yet
- Mid-Year Examination, 2023 Science Year 7 1 HourDocument23 pagesMid-Year Examination, 2023 Science Year 7 1 HourAl-Hafiz Bin SajahanNo ratings yet
- BTL Info CNC ProgrammDocument132 pagesBTL Info CNC ProgrammdieulafaitNo ratings yet
- Amc 20-21Document33 pagesAmc 20-21Vasco M C SantosNo ratings yet
- Recetario TransistoresDocument23 pagesRecetario TransistoresTitán SotoNo ratings yet
- Art and Geography: Patterns in The HimalayaDocument30 pagesArt and Geography: Patterns in The HimalayaBen WilliamsNo ratings yet
- Timer Relay ERV-09Document1 pageTimer Relay ERV-09wal idNo ratings yet
- BHLP Year Long Plan Required English Medium 2023 24 Batch Final 991676721629413Document3 pagesBHLP Year Long Plan Required English Medium 2023 24 Batch Final 991676721629413A V GamingNo ratings yet
- Additive Manufacturing Objective QuestionsDocument7 pagesAdditive Manufacturing Objective Questionsmohammad shaqib100% (4)
- Assignment On Cholera: Submitted ToDocument17 pagesAssignment On Cholera: Submitted ToEhesanulHaqueSaifNo ratings yet
- Chemistry Mid Term Exam 2014Document8 pagesChemistry Mid Term Exam 2014Adham TamerNo ratings yet
- Marriage HalldocxDocument50 pagesMarriage HalldocxBalaji Kamalakannan100% (2)
- Komatsu Technical BrochurDocument7 pagesKomatsu Technical BrochurBenjamin MossoNo ratings yet
- Microsoft Word - IRN Fab Transfer PCN NoticeDocument22 pagesMicrosoft Word - IRN Fab Transfer PCN NoticeJadilson PradoNo ratings yet
- BLANCHARD-The Debate Over Laissez Faire, 1880-1914Document304 pagesBLANCHARD-The Debate Over Laissez Faire, 1880-1914fantasmaNo ratings yet
- Polynomial Transformations of Tschirnhaus, Bring and Jerrard4s++Document5 pagesPolynomial Transformations of Tschirnhaus, Bring and Jerrard4s++wlsvieiraNo ratings yet
- Design A Roller Coaster ProjectDocument4 pagesDesign A Roller Coaster Projectapi-3564628400% (1)
- Deld12070 CC18 GT 371 C CDocument1 pageDeld12070 CC18 GT 371 C CDEBASIS BARMANNo ratings yet
- 14 WosDocument6 pages14 WosATUL KURZEKARNo ratings yet
- Assignment 7 - Cocktail RecipiesDocument20 pagesAssignment 7 - Cocktail RecipiesDebjyoti BanerjeeNo ratings yet
- The Sea DevilDocument6 pagesThe Sea DevilRevthi SankerNo ratings yet
- Amies A 114 - 3Document17 pagesAmies A 114 - 3Syed Umar Farooq100% (1)
- Fantasy AGE - Spell SheetDocument2 pagesFantasy AGE - Spell SheetpacalypseNo ratings yet
- The World S Finest Ideas in Cooling!: A Division ofDocument4 pagesThe World S Finest Ideas in Cooling!: A Division ofChiragNo ratings yet
- Lcnews227 - Nexera SeriesDocument47 pagesLcnews227 - Nexera SeriesMuhammad RohmanNo ratings yet
- +chapter 6 Binomial CoefficientsDocument34 pages+chapter 6 Binomial CoefficientsArash RastiNo ratings yet