You might also like
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Normal and Pathological Bronchial Semiology: A Visual ApproachFrom EverandNormal and Pathological Bronchial Semiology: A Visual ApproachPierre Philippe BaldeyrouNo ratings yet
- Adult and Paediatric Oral/nasal suction guidelinesDocument13 pagesAdult and Paediatric Oral/nasal suction guidelinesRuby Dela RamaNo ratings yet
- Airway Management and Common ConditionsDocument34 pagesAirway Management and Common Conditionsrigo montejoNo ratings yet
- Guidelines for managing tracheal intubation in critically ill patientsDocument26 pagesGuidelines for managing tracheal intubation in critically ill patientsFemiko Panji AprilioNo ratings yet
- 1.3 AirwaysDocument30 pages1.3 Airwaysdr.baselnassarNo ratings yet
- COVID 19. 4 - 13 KashmerDocument42 pagesCOVID 19. 4 - 13 KashmerIshfaq GanaiNo ratings yet
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDocument2 pagesAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasNo ratings yet
- Difficult Airway Management: By: Bereket Habtamu Advisor: Leulayehu AkaluDocument72 pagesDifficult Airway Management: By: Bereket Habtamu Advisor: Leulayehu AkaluagatakassaNo ratings yet
- Airway Management For Induction of General Anesthesia - UpToDate - Be4225b0Document31 pagesAirway Management For Induction of General Anesthesia - UpToDate - Be4225b0Nitin TrivediNo ratings yet
- Addis Ababa University Faculty of Medicine Difficult Airway ManagementDocument54 pagesAddis Ababa University Faculty of Medicine Difficult Airway ManagementagatakassaNo ratings yet
- RAPID SEQUENCE INTUBATION TECHNIQUEDocument55 pagesRAPID SEQUENCE INTUBATION TECHNIQUElorkan19100% (1)
- Essential Airway SkillsDocument21 pagesEssential Airway SkillsNia WahyuniNo ratings yet
- Airway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongDocument9 pagesAirway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongErwinRamadhaniNo ratings yet
- Airway / Breathing ProtocolsDocument15 pagesAirway / Breathing ProtocolsSbarcea AurelNo ratings yet
- Rapid Sequence Intubation: BackgroundDocument8 pagesRapid Sequence Intubation: Backgroundmarsh86No ratings yet
- Guide to Adult Nasal and Oropharyngeal SuctionDocument14 pagesGuide to Adult Nasal and Oropharyngeal SuctionillirpohnimNo ratings yet
- 2022 Preoperative Assessment Premedication Perioperative DocumentationDocument38 pages2022 Preoperative Assessment Premedication Perioperative DocumentationMohmmed Mousa100% (1)
- Airway AssessmentDocument26 pagesAirway AssessmentShehan WijayasiriwardanaNo ratings yet
- Anesthesia ChecklistsDocument50 pagesAnesthesia ChecklistsMark HindleNo ratings yet
- Difficult Airway Management During Anesthesia A Review of The Incidence and SolutionsDocument6 pagesDifficult Airway Management During Anesthesia A Review of The Incidence and SolutionsSudar Pecinta ParawaliNo ratings yet
- Chest Drains GuidanceDocument14 pagesChest Drains Guidancenob2011nobNo ratings yet
- Airway Management Inside and Outside Operating Rooms 2018 British Journal ofDocument3 pagesAirway Management Inside and Outside Operating Rooms 2018 British Journal ofSeveNNo ratings yet
- Airway Management Saq 47Document47 pagesAirway Management Saq 47RaMy “MhMd” ElaRabyNo ratings yet
- Walls 8093 CH 01Document7 pagesWalls 8093 CH 01Adriana MartinezNo ratings yet
- Management of Difficult AirwayDocument38 pagesManagement of Difficult AirwaySanjeewa de AlwisNo ratings yet
- Guidelines For The Insertion and Management of Chest Drains: WWW - Dbh.nhs - UkDocument14 pagesGuidelines For The Insertion and Management of Chest Drains: WWW - Dbh.nhs - UkStevanysungNo ratings yet
- Protocols AsesmenDocument290 pagesProtocols AsesmenDedelNo ratings yet
- Airway Management in TraumaDocument9 pagesAirway Management in TraumaAnonymous h0DxuJTNo ratings yet
- Symposium Papers: Emergency Airway ManagementDocument10 pagesSymposium Papers: Emergency Airway Managementdewin21No ratings yet
- QS EndotrachealIntubationDocument4 pagesQS EndotrachealIntubationChandra HalimNo ratings yet
- Vaishali Syal Moderator - Prof. J. R. ThakurDocument34 pagesVaishali Syal Moderator - Prof. J. R. ThakurTasha NurfitrianiNo ratings yet
- Prone Position Guidelines-2Document14 pagesProne Position Guidelines-2SAMINo ratings yet
- Emergency Airway and Ventilation-The Difficult Airway: By: Darryl Jamison Nremt-PDocument42 pagesEmergency Airway and Ventilation-The Difficult Airway: By: Darryl Jamison Nremt-Pccra 2019No ratings yet
- Endotracheal TubeDocument19 pagesEndotracheal TubeSarvess Muniandy100% (1)
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDocument11 pagesComplications of Endotracheal Intubation and Other Airway Management ProceduresashajangamNo ratings yet
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDocument11 pagesComplications of Endotracheal Intubation and Other Airway Management ProceduresSuresh Kumar100% (1)
- Airway 1Document6 pagesAirway 1Ilyes FerenczNo ratings yet
- %pediatric TracheostomyDocument25 pages%pediatric TracheostomyFabian Camelo OtorrinoNo ratings yet
- Airway ObstructionDocument7 pagesAirway ObstructionnesredeNo ratings yet
- Airway Technique Strengths and LimitationsDocument15 pagesAirway Technique Strengths and LimitationsJEFFERSON MUÑOZNo ratings yet
- Atls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryDocument55 pagesAtls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryAndris TapaNo ratings yet
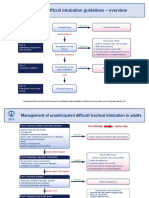
- Difficult Intubation Guidelines OverviewDocument3 pagesDifficult Intubation Guidelines OverviewMaufer AlNo ratings yet
- Airway Management - StatPearls - NCBI BookshelfDocument7 pagesAirway Management - StatPearls - NCBI BookshelfClarithq LengguNo ratings yet
- Endotracheal SuctionDocument11 pagesEndotracheal SuctionKeshav Singhmaar AryaNo ratings yet
- Concious Sedation PedoDocument29 pagesConcious Sedation PedodrkameshNo ratings yet
- Approach in Trauma Patient - OrthopaedicDocument91 pagesApproach in Trauma Patient - OrthopaedicBesi TuaNo ratings yet
- 2014 The ANZICS Percutaneous Dilatational Tracheostomy Consensus StatementDocument25 pages2014 The ANZICS Percutaneous Dilatational Tracheostomy Consensus StatementyudiNo ratings yet
- Medical Emergency Oral Q.docx26.docx8Document44 pagesMedical Emergency Oral Q.docx26.docx8Simina ÎntunericNo ratings yet
- Preoperative EvaluationDocument47 pagesPreoperative EvaluationCzerwin Juales100% (2)
- Awake Tracheal Intubation 2023Document13 pagesAwake Tracheal Intubation 2023Gabriela TeránNo ratings yet
- Airway ManagementDocument2 pagesAirway ManagementmedsmracelisNo ratings yet
- Imedpub Journals 2018 2018Document6 pagesImedpub Journals 2018 2018jemyNo ratings yet
- BTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Document21 pagesBTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Madalina TalpauNo ratings yet
- Oral Board Exam AudioDocument64 pagesOral Board Exam AudioMahjong SirenNo ratings yet
- Airway 2Document36 pagesAirway 2Daniel Dwi NugrohoNo ratings yet
- Oakes ACCSDocument167 pagesOakes ACCSKramer ChangNo ratings yet
- A Reading On Malpositioning of Supraglottic Airway DevicesDocument20 pagesA Reading On Malpositioning of Supraglottic Airway DevicesErnestine A. SambasNo ratings yet
- Emergency Tracheal Intubation Immediately Following Traumatic Injury An Eastern Association For The Surgery of Trauma Practice ManagementDocument11 pagesEmergency Tracheal Intubation Immediately Following Traumatic Injury An Eastern Association For The Surgery of Trauma Practice ManagementMadalina TalpauNo ratings yet
- Presenter: Jasmine Ngui Supervisor: DR AminDocument19 pagesPresenter: Jasmine Ngui Supervisor: DR AminNur Amin MuhammadNo ratings yet
- Coagulation Cascade: Presenter: Muhammad Nur Amin Bin Abd Rahman Supervisor: DR Muhammad Zihni Bin AbdullahDocument32 pagesCoagulation Cascade: Presenter: Muhammad Nur Amin Bin Abd Rahman Supervisor: DR Muhammad Zihni Bin AbdullahNur Amin MuhammadNo ratings yet
- Blood and Blood Products: Presenter: TAN LI LIAN Supervisor: DR AMINDocument15 pagesBlood and Blood Products: Presenter: TAN LI LIAN Supervisor: DR AMINNur Amin MuhammadNo ratings yet
- Fluids, Blood and Blood Products ManagementDocument19 pagesFluids, Blood and Blood Products ManagementNur Amin MuhammadNo ratings yet
- Limited Uretheral Mobilization Procedure (Lump) For Distal Penile Hypospadias Repair, A Single Centre Retrospective AnalysisDocument9 pagesLimited Uretheral Mobilization Procedure (Lump) For Distal Penile Hypospadias Repair, A Single Centre Retrospective AnalysisIJAR JOURNALNo ratings yet
- Drug Metabolism-LectDocument35 pagesDrug Metabolism-LectFiona OyatsiNo ratings yet
- Paper 2 Digestive SYSTEM WorksheeetDocument8 pagesPaper 2 Digestive SYSTEM WorksheeetOmar AlfrouhNo ratings yet
- Genetic Disorders: Chromosomal Abnormalities and Down SyndromeDocument27 pagesGenetic Disorders: Chromosomal Abnormalities and Down SyndromeMerwan KemalNo ratings yet
- Prenatal Development and Birth: The Developing Person Through The Life Span Kathleen Stassen Berger - Tenth EditionDocument42 pagesPrenatal Development and Birth: The Developing Person Through The Life Span Kathleen Stassen Berger - Tenth EditionJoel PayneNo ratings yet
- Gen 2 - Unit Test - 25.2.2022Document8 pagesGen 2 - Unit Test - 25.2.2022Phương Thảo NguyễnNo ratings yet
- A Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceDocument26 pagesA Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceCaio CesarNo ratings yet
- Cataract Qustion and AnswersDocument90 pagesCataract Qustion and AnswersVaishnavi MNo ratings yet
- Arthritis OsteoarthritisDocument43 pagesArthritis OsteoarthritisMYMANo ratings yet
- Class Test 3Document3 pagesClass Test 3Balakrishnan MarappanNo ratings yet
- A Survey On Data Mining Techniques For COVID PredictionDocument6 pagesA Survey On Data Mining Techniques For COVID PredictionWARSE Journals100% (2)
- Guidelines For Case Classification For The National Birth Defects Prevention StudyDocument9 pagesGuidelines For Case Classification For The National Birth Defects Prevention Studyjorge davidNo ratings yet
- 2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Document11 pages2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Anggi RiyaniNo ratings yet
- Mark Anthony A. Tom, M.D. First Year Internal Medicine Resident Davao Doctors HospitalDocument55 pagesMark Anthony A. Tom, M.D. First Year Internal Medicine Resident Davao Doctors HospitalMark Anthony TomNo ratings yet
- TRAFFIC JAM in EVERESTDocument18 pagesTRAFFIC JAM in EVERESTSB100% (1)
- The Psychology of Ageing - An Introduction, 3rd EdDocument320 pagesThe Psychology of Ageing - An Introduction, 3rd Edfauziahfasya123No ratings yet
- Resusciation Equipments in IcuDocument29 pagesResusciation Equipments in Icuvinoli100% (1)
- Physical Fitness Physical FitnessDocument18 pagesPhysical Fitness Physical FitnessCharmaine JanorasNo ratings yet
- Rizal To Paris To GermanyDocument48 pagesRizal To Paris To Germanybenj panganibanNo ratings yet
- 1 PBDocument11 pages1 PBNaswa Alifia PutriNo ratings yet
- Statistical vs clinical significanceDocument38 pagesStatistical vs clinical significanceGeorge StoicaNo ratings yet
- Cram Reviewer MusculoskeletalDocument32 pagesCram Reviewer MusculoskeletalGwynthselle SalazarNo ratings yet
- Understand the Difference Between Omega-3 EPA and DHADocument7 pagesUnderstand the Difference Between Omega-3 EPA and DHASutanto TanakaNo ratings yet
- Activity - Nutrition On The Internet Worksheet 3Document2 pagesActivity - Nutrition On The Internet Worksheet 3Carlo FernandoNo ratings yet
- Session 10. Review of Centric Records RECORDSDocument25 pagesSession 10. Review of Centric Records RECORDSbaraa.abdulrahman.23No ratings yet
- Lif Vis Pol Intp Unit 3b-300dpiDocument6 pagesLif Vis Pol Intp Unit 3b-300dpin6wr95xtmjNo ratings yet
- Og - Applying To The Ndis v5.0 Approved - External 2023-09-28Document55 pagesOg - Applying To The Ndis v5.0 Approved - External 2023-09-28faithgaye432No ratings yet
- Clinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and PapacarieDocument8 pagesClinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and PapacarieVianney Guadalupe González ElizaldeNo ratings yet
- Cardiopulmonary Resuscitation Update: Continuing Education ColumnDocument9 pagesCardiopulmonary Resuscitation Update: Continuing Education Columnkang soon cheolNo ratings yet
- Khatib2017 PDFDocument14 pagesKhatib2017 PDFluxmansrikanthaNo ratings yet