You might also like
- Distal Radius FracturesDocument68 pagesDistal Radius Fracturescalvin_c_wangNo ratings yet
- Lect 8 - Internal Fixation - IIDocument21 pagesLect 8 - Internal Fixation - IIAnkit LakshyaNo ratings yet
- Acetabulum AOSR ENGDocument48 pagesAcetabulum AOSR ENGAdil SultaniNo ratings yet
- FracturePPT UpdatedDocument108 pagesFracturePPT Updatedgaile pattugalanNo ratings yet
- Colles Fracture & Knee DislocationDocument38 pagesColles Fracture & Knee DislocationNap91No ratings yet
- Femur Leg FracturesDocument78 pagesFemur Leg FracturesAnonymous hTivgzixVNNo ratings yet
- Ankle Instability: Dr. Syarif Hidayatullah, SP - OT, M.KesDocument75 pagesAnkle Instability: Dr. Syarif Hidayatullah, SP - OT, M.Kesahmad zakyNo ratings yet
- Ankle InjuriesDocument32 pagesAnkle InjuriesArefa PandorNo ratings yet
- Pelvic and Lower LimbDocument87 pagesPelvic and Lower Limbwanni wuyamNo ratings yet
- Intertrochanter Femur Fracture: M.Akhyar Baharuddin 20194010011Document23 pagesIntertrochanter Femur Fracture: M.Akhyar Baharuddin 20194010011Muhammad AkhyarNo ratings yet
- Fracture FemurDocument28 pagesFracture FemurKulsoom ShahNo ratings yet
- Tibial Plateau FractureDocument7 pagesTibial Plateau FractureHerryanto AgustriadiNo ratings yet
- Fractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaDocument50 pagesFractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaJustin Ahorro-DionisioNo ratings yet
- Blue Writing Is What I Added To These Notes: RadiographyDocument46 pagesBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Lower Limb FracturesDocument124 pagesLower Limb FracturesMaríaJosé Dip100% (3)
- ANKLE FRACTURE CLASSIFICATION AND TREATMENTDocument47 pagesANKLE FRACTURE CLASSIFICATION AND TREATMENTAbhishek UpadhyayNo ratings yet
- 12 - Fractures & Dislocations of The Upper Limb-1Document84 pages12 - Fractures & Dislocations of The Upper Limb-1Ain Ul NoorNo ratings yet
- Femur Injuries and Fractures Guide: Causes, Symptoms, TreatmentDocument23 pagesFemur Injuries and Fractures Guide: Causes, Symptoms, Treatmentchelle_morales26No ratings yet
- Definition: Is A Condition Resulting in Partial or Complete Separation of A Segment of Normal Hyaline Cartilage From It's Supporting BoneDocument8 pagesDefinition: Is A Condition Resulting in Partial or Complete Separation of A Segment of Normal Hyaline Cartilage From It's Supporting BoneKarla Chariz Fernandez BayagNo ratings yet
- Elbow Joint Injuries - Assessment & TreatmentDocument55 pagesElbow Joint Injuries - Assessment & TreatmentSushma ImmadiNo ratings yet
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDocument90 pagesFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahNo ratings yet
- Lower Limb InjuriesDocument47 pagesLower Limb InjuriesDaisyyhyNo ratings yet
- Treatment of Femur FracturesDocument55 pagesTreatment of Femur FracturesMabvuto BandaNo ratings yet
- Ankle Fractures - StatPearls - NCBI BookshelfDocument12 pagesAnkle Fractures - StatPearls - NCBI Bookshelfbhushan adhariNo ratings yet
- Orthopedic RSUD Panembahan Senopati BantulDocument28 pagesOrthopedic RSUD Panembahan Senopati Bantulwinda alviraNo ratings yet
- Affections of The KneeDocument92 pagesAffections of The KneeJudy Ann Bahom SantiagoNo ratings yet
- Long Bone Fracture Management - Dr. ImanDocument20 pagesLong Bone Fracture Management - Dr. ImanYuliusNo ratings yet
- Fractures: (On Which We Will Likely Be Pimped)Document66 pagesFractures: (On Which We Will Likely Be Pimped)Marivic DianoNo ratings yet
- Orthopedic InjuriesDocument27 pagesOrthopedic InjuriesvikramNo ratings yet
- Patient - Co.uk - Trusted Medical Information and Support: Knee Fractures and DislocationsDocument4 pagesPatient - Co.uk - Trusted Medical Information and Support: Knee Fractures and DislocationsHayelom MichaelNo ratings yet
- Elbow Dislocation: DR Ajith John KDocument53 pagesElbow Dislocation: DR Ajith John KPankaj VatsaNo ratings yet
- Risks, Causes, Symptoms & Treatment of Acquired Hip DislocationDocument1 pageRisks, Causes, Symptoms & Treatment of Acquired Hip DislocationZul IsmailNo ratings yet
- Upper Limb Fracture GuideDocument90 pagesUpper Limb Fracture Guideatikah_jamilNo ratings yet
- Ankle Joint InjuriesDocument23 pagesAnkle Joint InjuriesSafeer VarkalaNo ratings yet
- Joint DislocationsDocument64 pagesJoint DislocationsSabrina Indri WardaniNo ratings yet
- Frienchzel Joy A. Asis Group 3 BSN 3-ADocument14 pagesFrienchzel Joy A. Asis Group 3 BSN 3-AKenneth Louis GalizaNo ratings yet
- Internal Derangements of the Knee (IDK): Causes, Symptoms & TreatmentDocument92 pagesInternal Derangements of the Knee (IDK): Causes, Symptoms & TreatmentAzad Roxo100% (3)
- Thoracolumbar Spine Trauma Classification and ManagementDocument29 pagesThoracolumbar Spine Trauma Classification and ManagementFernaldi Anggadha100% (1)
- Dr. Abdul Qadir P.G Orthopedic Trainee C.H.K: Intertrochanteric Fractures of The FemurDocument21 pagesDr. Abdul Qadir P.G Orthopedic Trainee C.H.K: Intertrochanteric Fractures of The FemurAbdul QadirNo ratings yet
- C14 - Coloana Vertebrala Engleza 2Document109 pagesC14 - Coloana Vertebrala Engleza 2Andreea DanielaNo ratings yet
- Spinal Trauma Guide Under 40 CharactersDocument80 pagesSpinal Trauma Guide Under 40 CharactersMuhammad YaminNo ratings yet
- Shoulder Trauma Fractures and Dislocations-Orthoinfo - AaosDocument6 pagesShoulder Trauma Fractures and Dislocations-Orthoinfo - Aaosapi-228773845No ratings yet
- Orthopedic Surgery: Fracture and DislocationDocument8 pagesOrthopedic Surgery: Fracture and DislocationAhmad Samim AfsharNo ratings yet
- Orthopedic: Compression FracturesDocument7 pagesOrthopedic: Compression FracturesArianne LaviñaNo ratings yet
- Ankle Fractures: Dr. T. VikramDocument35 pagesAnkle Fractures: Dr. T. VikramVicky VikramNo ratings yet
- Elbow Injuries and FracturesDocument9 pagesElbow Injuries and FracturesJyoti MaheshwariNo ratings yet
- NCP: Nursing Care Plan For Bone FracturesDocument8 pagesNCP: Nursing Care Plan For Bone FracturesElham TabaoNo ratings yet
- Radial Head FractureDocument40 pagesRadial Head FractureammarNo ratings yet
- Hip FracturesDocument74 pagesHip FracturesMina SamirNo ratings yet
- Hip fracture causes, symptoms and treatmentDocument4 pagesHip fracture causes, symptoms and treatmentJoel Vertt C. Balboa100% (1)
- Proximal Femur Fractures: Neck, Trochanteric & Subtrochanteric InjuriesDocument38 pagesProximal Femur Fractures: Neck, Trochanteric & Subtrochanteric InjuriesMisoNo ratings yet
- Joints of Lower LimbDocument7 pagesJoints of Lower LimbjsdlzjNo ratings yet
- 10-ankle jointDocument19 pages10-ankle jointadham.hanyNo ratings yet
- Trauma Musculoskeletal of Truncus: Spinal Fracture and TypesDocument13 pagesTrauma Musculoskeletal of Truncus: Spinal Fracture and TypesDewi AtmiyantiNo ratings yet
- Lecture 7 Upper Limb FracturesDocument43 pagesLecture 7 Upper Limb Fracturesmukhtar abddiNo ratings yet
- Alterations Related To Musculoskeletal Trauma: Lisa M. Dunn MSN/Ed, RN, CCRN, CNEDocument83 pagesAlterations Related To Musculoskeletal Trauma: Lisa M. Dunn MSN/Ed, RN, CCRN, CNEjayvee2012No ratings yet
- Deforming Force in Lower Limb Fracture FixDocument28 pagesDeforming Force in Lower Limb Fracture FixRizki Setiawan SultanNo ratings yet
- Hip Joint DislocationDocument19 pagesHip Joint Dislocationshaoib.grandyNo ratings yet
- Orthopedics Notes for Medical StudentsFrom EverandOrthopedics Notes for Medical StudentsRating: 4.5 out of 5 stars4.5/5 (3)
- Insurance Fraud PPT (Final)Document30 pagesInsurance Fraud PPT (Final)Gaurav Savlani83% (6)
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- A Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreDocument11 pagesA Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreRamasamyNagarajan100% (1)
- Child Abuse Research JournalDocument9 pagesChild Abuse Research JournaladrianekattnerNo ratings yet
- VGEC 2024_Thư mời hội nghịDocument8 pagesVGEC 2024_Thư mời hội nghịkhongquantam101010No ratings yet
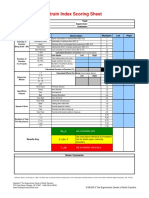
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- EGZOTech Luna EMG Brochure 2018 With LogoDocument13 pagesEGZOTech Luna EMG Brochure 2018 With LogoApostolis KopoukisNo ratings yet
- Marihuana EsquizofreniaDocument30 pagesMarihuana EsquizofreniaJ Elver SilvaNo ratings yet
- ICICI Bank Mortgage - HS360 Product FinalDocument29 pagesICICI Bank Mortgage - HS360 Product FinalRishu GiriNo ratings yet
- Unit 1-Omd553-Telehealth TechnologyDocument53 pagesUnit 1-Omd553-Telehealth TechnologyjgjeslinNo ratings yet
- Designsolutions 2010springDocument68 pagesDesignsolutions 2010springjkarpitskiyNo ratings yet
- Careers Surrey 20181Document15 pagesCareers Surrey 20181Kevin_Nguyen117No ratings yet
- Effects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged CyclingDocument9 pagesEffects of Energy Gel Ingestion On Blood Glucose, Lactate, and Performance Measures During Prolonged Cyclingjose david HerreraNo ratings yet
- Anatomia SufletuluiDocument1 pageAnatomia SufletuluiAlexandrina DeaşNo ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- Sdbiosensor Insert F D DimerDocument2 pagesSdbiosensor Insert F D DimerEmi SoubaiNo ratings yet
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet
- Municipality of Naic, Cavite Gender and Development Plan: Programs / Projects / Activities Appropriation ObligationDocument2 pagesMunicipality of Naic, Cavite Gender and Development Plan: Programs / Projects / Activities Appropriation Obligationbunso2012No ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Que No4 & 5-With Clues and Without CluesDocument4 pagesQue No4 & 5-With Clues and Without CluesMir Yamin Uddin ZidanNo ratings yet
- PDF Biaya MaternityDocument2 pagesPDF Biaya MaternityKurnia Yuliyanti RahayuNo ratings yet
- Understanding patients' and healthcare providers' confidentiality rights and obligationsDocument2 pagesUnderstanding patients' and healthcare providers' confidentiality rights and obligationsMelody B. MiguelNo ratings yet
- Canine-Assisted Occupational Therapy For Children On The Autism Spectrum: Parents' PerspectivesDocument10 pagesCanine-Assisted Occupational Therapy For Children On The Autism Spectrum: Parents' PerspectivesDaniele PendezaNo ratings yet
- The30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Document17 pagesThe30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Alexander OrzocoNo ratings yet
- Antiglobulin TestDocument28 pagesAntiglobulin TestAvi Verma100% (1)
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- Kurukshetra University PhD Entrance Exam GuideDocument27 pagesKurukshetra University PhD Entrance Exam GuidemanojrkmNo ratings yet
- Thomas Foot ReflexologyDocument112 pagesThomas Foot ReflexologySa MiNo ratings yet
- Press Final - Abstract Book PDFDocument157 pagesPress Final - Abstract Book PDFAmbesh JhaNo ratings yet
- Intern Performance Review TemplateDocument3 pagesIntern Performance Review TemplatePrincess Joan InguitoNo ratings yet