You might also like
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
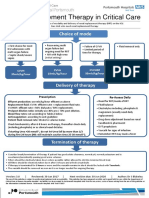
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- Low Molecular Weight Heparins (LMWH) : I. Mechanism of ActionDocument7 pagesLow Molecular Weight Heparins (LMWH) : I. Mechanism of ActionIniya RajendranNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- Most of Cardiac Care Unit (C.C.U) DrugsDocument57 pagesMost of Cardiac Care Unit (C.C.U) DrugsOsama OmarNo ratings yet
- Bivalirudine Drug Presentation From Nicvd DhakaDocument28 pagesBivalirudine Drug Presentation From Nicvd DhakaNavojit ChowdhuryNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Initial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentDocument3 pagesInitial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentLamNo ratings yet
- Anticoagulant Pocket GuideDocument8 pagesAnticoagulant Pocket GuideDrew John Minardi100% (2)
- Anticoagulation PharmacologyDocument36 pagesAnticoagulation PharmacologyaymenNo ratings yet
- Heparin Drip ProtocolDocument16 pagesHeparin Drip Protocolapi-277534147100% (1)
- Nifedipine Drug ProfileDocument8 pagesNifedipine Drug ProfileM NoumanNo ratings yet
- An Introduction To Obstetrical Emergencies: Charles D Giordano CRNA, MSNDocument49 pagesAn Introduction To Obstetrical Emergencies: Charles D Giordano CRNA, MSNEffendi ZakriNo ratings yet
- Dha Pharmacist Examination Questions 9 JULY 2021Document6 pagesDha Pharmacist Examination Questions 9 JULY 2021Naveen KarankaraNo ratings yet
- HeparinDocument1 pageHeparinRatna Sari DewiNo ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNo ratings yet
- Hip Fracture GuidelinesDocument10 pagesHip Fracture GuidelinesiamseraNo ratings yet
- Heparin Infusion Guideline PDFDocument3 pagesHeparin Infusion Guideline PDFbrigde_xNo ratings yet
- Drug LipitorDocument1 pageDrug LipitorSrkocherNo ratings yet
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- Cilastati Imipenem Drug InfoDocument19 pagesCilastati Imipenem Drug InfoCosmina GeorgianaNo ratings yet
- Agatha Christie - Craciunul Lui PoirotDocument14 pagesAgatha Christie - Craciunul Lui PoirotIokan DanNo ratings yet
- 1614978209sampleDocument9 pages1614978209sampleReddyNo ratings yet
- PRE ANAESTHETIC ASSESSMENT New 1Document41 pagesPRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyNo ratings yet
- COVID-19 Quick Reference Guide for Drugs & TreatmentDocument1 pageCOVID-19 Quick Reference Guide for Drugs & TreatmentBoules AtefNo ratings yet
- Print 18Document4 pagesPrint 18Mahmoud SelimNo ratings yet
- MC HeparinDocument7 pagesMC HeparinCliff by the seaNo ratings yet
- Anticoagulatio N Asra Guidelines: Sravya VemuriDocument62 pagesAnticoagulatio N Asra Guidelines: Sravya VemuriSiva Prasad AspNo ratings yet
- Anticoagulation Monitoring Hand-OutDocument69 pagesAnticoagulation Monitoring Hand-OutApril OcampoNo ratings yet
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095No ratings yet
- Bevacizumab Carboplatin Paclitaxel For Cervical Cancers CRP14GY017 v1.0Document6 pagesBevacizumab Carboplatin Paclitaxel For Cervical Cancers CRP14GY017 v1.0andibarosNo ratings yet
- Ibutilide FumarateDocument3 pagesIbutilide Fumarateapi-3797941No ratings yet
- Unfractionate Heparin Low Molecular Weight HeparinDocument3 pagesUnfractionate Heparin Low Molecular Weight HeparinArun KumarNo ratings yet
- Atropine: Version 2: Published 2/2021. Review 2/2024Document1 pageAtropine: Version 2: Published 2/2021. Review 2/2024gugicevdzoceNo ratings yet
- Acetyl Cyst EineDocument4 pagesAcetyl Cyst Einemauran aurodNo ratings yet
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- Ketorolac (Systemic) - Drug Information - UpToDateDocument42 pagesKetorolac (Systemic) - Drug Information - UpToDateJosué Pablo Chicaiza AbadNo ratings yet
- Acs 02152022 CjangDocument2 pagesAcs 02152022 Cjangapi-611971572No ratings yet
- ASRA Guidelines on Neuraxial Blockade and AnticoagulantsDocument66 pagesASRA Guidelines on Neuraxial Blockade and AnticoagulantsAshiyan IrfanNo ratings yet
- STD Heparin Protocol MethodistDocument1 pageSTD Heparin Protocol Methodistd40sithuiNo ratings yet
- Deep Vein ThrombosisDocument22 pagesDeep Vein ThrombosisEznal MahidinNo ratings yet
- Anticoagulation Dosing Recommendations COVID 19 PatientsDocument1 pageAnticoagulation Dosing Recommendations COVID 19 PatientsChalwe HowardNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Heparin Vs Warfarin (Coumadin)Document5 pagesHeparin Vs Warfarin (Coumadin)blankNo ratings yet
- Fac Thrombolysis 2007Document36 pagesFac Thrombolysis 2007Tri Harjono0% (1)
- ACS ManagementDocument24 pagesACS ManagementkalfNo ratings yet
- Enoxaparin MAGDocument2 pagesEnoxaparin MAGmlbrown8No ratings yet
- Read Me: Route 159 Open SansDocument19 pagesRead Me: Route 159 Open SansEndangWulanSariNo ratings yet
- Acute Myocardial Infarction: Recognition and AssessmentDocument7 pagesAcute Myocardial Infarction: Recognition and AssessmentHasnainKhimjiNo ratings yet
- Acetylcysteine - Drug Information - UpToDateDocument22 pagesAcetylcysteine - Drug Information - UpToDateDaniel ChávezNo ratings yet
- Pharmacology CardiovascularDocument86 pagesPharmacology Cardiovascularamasoud96 amasoud96No ratings yet
- Ovarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorDocument5 pagesOvarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorAnonymous g1hIPZNo ratings yet
- Propranolol HydrochlorideDocument8 pagesPropranolol HydrochlorideKrima PatelNo ratings yet
- Neuraxial Blockade and AnticoagulantsDocument69 pagesNeuraxial Blockade and Anticoagulantskamel6No ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Teaching Experience LogDocument2 pagesTeaching Experience Logapi-668470097No ratings yet
- CV UpdatedDocument7 pagesCV Updatedapi-668470097No ratings yet
- Sterile Products Lab ManualsDocument5 pagesSterile Products Lab Manualsapi-668470097No ratings yet
- Chronic Kidney DiseaseDocument3 pagesChronic Kidney Diseaseapi-668470097No ratings yet
- Blood Groups, Abo and RHDocument6 pagesBlood Groups, Abo and RHromeoenny4154No ratings yet
- ISUOG Basic Training: Gynecological Ultrasound: The BasicsDocument34 pagesISUOG Basic Training: Gynecological Ultrasound: The BasicsTheodoraAlinaNo ratings yet
- Peterson S Master TOEFL VocabularyDocument209 pagesPeterson S Master TOEFL Vocabularydnguyen_25254486% (14)
- Ceramic in DentistryDocument6 pagesCeramic in DentistryDilesh PradhanNo ratings yet
- Unit 8 Comprehension Quiz - T. PhangDocument3 pagesUnit 8 Comprehension Quiz - T. PhangPhang SouNo ratings yet
- Freediving Article PDFDocument4 pagesFreediving Article PDFdoha73039944100% (1)
- HypersensitivityDocument38 pagesHypersensitivityMilan KcNo ratings yet
- Yoga Healthy Heart GuideDocument100 pagesYoga Healthy Heart GuidePralesh12No ratings yet
- Hagerman - Training The Energy SystemsDocument8 pagesHagerman - Training The Energy Systemsmkn1214100% (1)
- Autism Spectrum Disorder Screening Machine Learning Adaptation and DSM 5 Fulfillment PDFDocument6 pagesAutism Spectrum Disorder Screening Machine Learning Adaptation and DSM 5 Fulfillment PDFBudi SantoNo ratings yet
- Multicultural Lesson PlanDocument6 pagesMulticultural Lesson Planapi-331853863No ratings yet
- Applied Paramedic Law and Ethic - Townsend & LuckDocument362 pagesApplied Paramedic Law and Ethic - Townsend & LuckCherie Harward100% (3)
- Self Care Handout-1Document3 pagesSelf Care Handout-1Wandarh RhNo ratings yet
- Radiodiagnostik Dan RadioterapiDocument81 pagesRadiodiagnostik Dan RadioterapiYuu Ayu'k LifestarNo ratings yet
- GoniosDocument14 pagesGoniosJayricDepalobosNo ratings yet
- Varcarolis: Essentials of Psychiatric Mental Health Nursing: Test Bank Chapter 10: Personality Disorders Multiple ChoiceDocument17 pagesVarcarolis: Essentials of Psychiatric Mental Health Nursing: Test Bank Chapter 10: Personality Disorders Multiple Choiceyaneidys perezNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Resistensi AntibiotikDocument21 pagesResistensi AntibiotikMaruliTuaNo ratings yet
- Analysus of The Soft Tissue Profile in Croatians With Normal Occlusions and Well-Balanced FacesDocument6 pagesAnalysus of The Soft Tissue Profile in Croatians With Normal Occlusions and Well-Balanced FacesIvanna H. A.No ratings yet
- The Pittston Dispatch 08-05-2012Document62 pagesThe Pittston Dispatch 08-05-2012The Times LeaderNo ratings yet
- Yimi Catalogue2014Document60 pagesYimi Catalogue2014ariovaldofjNo ratings yet
- Cytochemistry Chapter SummaryDocument3 pagesCytochemistry Chapter SummaryNathaniel SimNo ratings yet
- Journal PediaDocument2 pagesJournal PediapeteiroNo ratings yet
- Potassium ChlorideDocument2 pagesPotassium ChlorideRene John FranciscoNo ratings yet
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- AP2 Unit 6 Exam Review CASDocument12 pagesAP2 Unit 6 Exam Review CASMarera DomnicNo ratings yet
- Gharama Za Matibabu PKP Kituo Cha AfyaDocument14 pagesGharama Za Matibabu PKP Kituo Cha AfyashaggyzegratNo ratings yet
- ECG for Beginners: A Concise Guide to ECG Terminology and InterpretationDocument66 pagesECG for Beginners: A Concise Guide to ECG Terminology and InterpretationblndfflNo ratings yet
- FISIOLOGI HORMON TIROIDDocument54 pagesFISIOLOGI HORMON TIROIDaan SyamhaNo ratings yet
- WHO Analgesic Ladder GuideDocument25 pagesWHO Analgesic Ladder Guideayanle Abdi Ali100% (1)