You might also like
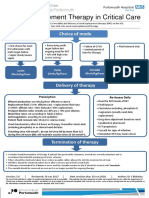
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- VTE_prophylaxis_PROTOCOL _V1.1_with Forms_07_Dec_2023Document20 pagesVTE_prophylaxis_PROTOCOL _V1.1_with Forms_07_Dec_2023hatem newishyNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- VTE_prophylaxis_PROTOCOL_V1.2_withForms_31_Dec_2023Document19 pagesVTE_prophylaxis_PROTOCOL_V1.2_withForms_31_Dec_2023hatem newishyNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- BPaL L Webinar (002) - 231128 - 174942Document27 pagesBPaL L Webinar (002) - 231128 - 174942AkshayKumarSinghNo ratings yet
- Low Molecular Weight Heparins (LMWH) : I. Mechanism of ActionDocument7 pagesLow Molecular Weight Heparins (LMWH) : I. Mechanism of ActionIniya RajendranNo ratings yet
- 1 - New Drug Update 2015 - FINALEBDocument62 pages1 - New Drug Update 2015 - FINALEBnikhilNo ratings yet
- VTE-Prophylaxis-Protocol - MOHDocument13 pagesVTE-Prophylaxis-Protocol - MOHreham ONo ratings yet
- Venous Thromboembolism With Blanks ResidentsDocument9 pagesVenous Thromboembolism With Blanks Residentsapi-648714317No ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- AIIMS issues new guidelines for treatment of Covid-19 casesDocument7 pagesAIIMS issues new guidelines for treatment of Covid-19 casessenthil kumarNo ratings yet
- Anticoagulation strategies for COVID-19 patients at BMCDocument1 pageAnticoagulation strategies for COVID-19 patients at BMCAvinash KumbharNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- University of Maryland Medical Center Fluconazole (Diflucan®)Document6 pagesUniversity of Maryland Medical Center Fluconazole (Diflucan®)damondouglasNo ratings yet
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- Protect ICU Patients From Harm With DVT, Stress Ulcer, and VAP PreventionDocument1 pageProtect ICU Patients From Harm With DVT, Stress Ulcer, and VAP PreventionMohammedNo ratings yet
- COVID Therapeutics: Steroids Benefit for Oxygen, Ventilated PatientsDocument9 pagesCOVID Therapeutics: Steroids Benefit for Oxygen, Ventilated PatientsStrahinja ŠkoboNo ratings yet
- Treatment of COVIDDocument2 pagesTreatment of COVIDGunduz AgaNo ratings yet
- Newer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineDocument57 pagesNewer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineMuhammad Reza FirdausNo ratings yet
- Anticoagulation Dosing Recommendations COVID 19 PatientsDocument1 pageAnticoagulation Dosing Recommendations COVID 19 PatientsChalwe HowardNo ratings yet
- Palliative care-MBODocument17 pagesPalliative care-MBOChonnikan LimpongsanurukNo ratings yet
- Anticoagulatio N Asra Guidelines: Sravya VemuriDocument62 pagesAnticoagulatio N Asra Guidelines: Sravya VemuriSiva Prasad AspNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Acs 2023 Part 4 Presentation VersionDocument38 pagesAcs 2023 Part 4 Presentation Versionapi-668470097No ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument11 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDPrashanta Barman Palas100% (1)
- COVID-19 Protocol by EVMSDocument13 pagesCOVID-19 Protocol by EVMSKrishnamurthi CG100% (1)
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- TablesDocument21 pagesTablesMélissa BlancNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- COVID-19 Treatment GuidelinesDocument26 pagesCOVID-19 Treatment GuidelinesStonefalconNo ratings yet
- UFH LMWH Fonda - 06september2020Document7 pagesUFH LMWH Fonda - 06september2020gabrimarteNo ratings yet
- Antibiotic Protocol 2018Document10 pagesAntibiotic Protocol 2018sumayyah995No ratings yet
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentDocument5 pagesHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVNo ratings yet
- Antibiotic Pocket GuideDocument19 pagesAntibiotic Pocket GuideNaomi Liang100% (1)
- Laboratory Confirmed Covid 19 Patient: Department of Health & Family Welfare, Govt of West BengalDocument2 pagesLaboratory Confirmed Covid 19 Patient: Department of Health & Family Welfare, Govt of West BengalSujoyDeNo ratings yet
- ACLS ModuleDocument68 pagesACLS ModuleSalah ElbadawyNo ratings yet
- Pediatric Acute Sepsis: Physician'S OrdersDocument4 pagesPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNo ratings yet
- COVID-19 Therapeutics for Healthcare WorkersDocument9 pagesCOVID-19 Therapeutics for Healthcare Workers[JC]No ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- DVT Prophylaxis Safety ContraindicatDocument1 pageDVT Prophylaxis Safety Contraindicata1b14No ratings yet
- Enoxaparin Guideline for Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin Guideline for Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Atrial Fibrillation TDDocument6 pagesAtrial Fibrillation TDapi-594366475No ratings yet
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Anti Cancer DrugsDocument29 pagesAnti Cancer DrugsFrances RamosNo ratings yet
- Lisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationDocument6 pagesLisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationCliff by the seaNo ratings yet
- Sweeney PDFDocument81 pagesSweeney PDFReitza RevilNo ratings yet
- Vasodilator and Anticoagulant Agents SummaryDocument23 pagesVasodilator and Anticoagulant Agents Summarymonyet65No ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNo ratings yet
- Drugs Study Neh Jai2xDocument10 pagesDrugs Study Neh Jai2xjai2xNo ratings yet
- Farmakologi Obat AntikoagulanDocument20 pagesFarmakologi Obat AntikoagulanHenderi SaputraNo ratings yet
- EC Epirubicin Cyclophosphamide Adjuvant Neo-Adjuvant Regimen Protocol V1.0Document5 pagesEC Epirubicin Cyclophosphamide Adjuvant Neo-Adjuvant Regimen Protocol V1.0smokkerNo ratings yet
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Neonatal HypertensionDocument21 pagesNeonatal HypertensionMuhammad Ammar Abdul WahabNo ratings yet
- Acute Pyelonephritis Treatment GuidelinesDocument4 pagesAcute Pyelonephritis Treatment GuidelinesPeter InocandoNo ratings yet
- Diagnose CKD:: ACE inhibitor/ARB UseDocument2 pagesDiagnose CKD:: ACE inhibitor/ARB UseAman AmanNo ratings yet
- Antenna Arrays NotesDocument26 pagesAntenna Arrays NotesBoules AtefNo ratings yet
- Antenna Basics PDFDocument24 pagesAntenna Basics PDFBoules AtefNo ratings yet
- Lecture05 MIT PDFDocument19 pagesLecture05 MIT PDFBoules AtefNo ratings yet
- Radiation Pattern of a Parallelogram Loop AntennaDocument8 pagesRadiation Pattern of a Parallelogram Loop AntennaMahima ArrawatiaNo ratings yet
- Tensor AlgebraDocument16 pagesTensor AlgebraBoules AtefNo ratings yet
- ResonanceDocument3 pagesResonanceBoules Atef0% (1)
- Loop and Helix AntennasDocument10 pagesLoop and Helix AntennasBoules AtefNo ratings yet
- Paper For Enzyme ActivityDocument7 pagesPaper For Enzyme ActivityFar hatNo ratings yet
- Topics Included:: Blue Print Parasitology SectionDocument7 pagesTopics Included:: Blue Print Parasitology SectionKaye HernandezNo ratings yet
- Vesicular Drug Delivery Systems A NovelDocument10 pagesVesicular Drug Delivery Systems A NovelJERIN REJINo ratings yet
- Aemses Sof Be LCP 2021 2022Document16 pagesAemses Sof Be LCP 2021 2022ROMEO SANTILLANNo ratings yet
- GastricDocument207 pagesGastricfavo riteNo ratings yet
- Atraumatic Restorative TreatmentDocument31 pagesAtraumatic Restorative TreatmentJude Aldo PaulNo ratings yet
- Contour User Guide 99C71529 BAR Eng 99C71529 Rev.7Document48 pagesContour User Guide 99C71529 BAR Eng 99C71529 Rev.7turijaNo ratings yet
- Cronic Kidney Disease: Prof. Dr. Agus Tessy SP - PD KGH Systema UrologiDocument39 pagesCronic Kidney Disease: Prof. Dr. Agus Tessy SP - PD KGH Systema UrologifauziyahabidahNo ratings yet
- 101 - 36903 - Chapter 14 HairDocument17 pages101 - 36903 - Chapter 14 HairAaromal MaanasNo ratings yet
- Protein-Calorie MalnutritionDocument25 pagesProtein-Calorie Malnutritionsajjad khanNo ratings yet
- Fibromyalgia: Annals of Internal MedicineDocument16 pagesFibromyalgia: Annals of Internal MedicineTeofanes PonceNo ratings yet
- Enderal Book CollectionDocument266 pagesEnderal Book CollectionMagazyn BotNo ratings yet
- Artificial Insemination and Infertility Management in Dairy AnimalsDocument80 pagesArtificial Insemination and Infertility Management in Dairy AnimalsИгор Галоски100% (1)
- Nipple Discharge 3Document3 pagesNipple Discharge 3Dima PathNo ratings yet
- Dermatology Atlas For Skin ColorDocument300 pagesDermatology Atlas For Skin ColorKiTty Kriss75% (8)
- DepEd LCP July3Document49 pagesDepEd LCP July3Jelai ApallaNo ratings yet
- Allergy - 2016 - Late Breaking Poster Session LB TPS 10 18Document42 pagesAllergy - 2016 - Late Breaking Poster Session LB TPS 10 18PATRICIANo ratings yet
- CSIR Life Sciences Official Model PaperDocument34 pagesCSIR Life Sciences Official Model PaperSoftqGunturNo ratings yet
- Hepatite B CoinfeçãoDocument31 pagesHepatite B Coinfeçãojefferson2392No ratings yet
- Angel Summer Field Report (Max Hospital)Document50 pagesAngel Summer Field Report (Max Hospital)varshasharma05100% (1)
- Reading Passages - TEST4Document21 pagesReading Passages - TEST4Bilgin AkbabaNo ratings yet
- Mind MagazineDocument36 pagesMind MagazineLauren Crociati100% (2)
- Unit 8 Stress and Its EffectsDocument14 pagesUnit 8 Stress and Its Effectsafiya chandNo ratings yet
- EmbryologyDocument26 pagesEmbryologyMeer BabanNo ratings yet
- Care RopDocument9 pagesCare RopYury RequeneNo ratings yet
- Gram Negative RodsDocument23 pagesGram Negative RodsYasir KareemNo ratings yet
- Chemical Handling ProcedureDocument15 pagesChemical Handling ProcedureGHULAM MOHYUDDINNo ratings yet
- CPH AssignmentDocument3 pagesCPH AssignmentChrystelle Mariano TibayNo ratings yet
- FaciitisDocument17 pagesFaciitisdalaginding clophNo ratings yet
- Lesson 2 Bacterial Identification and Processing ModuleDocument20 pagesLesson 2 Bacterial Identification and Processing ModuleTinNo ratings yet