You might also like
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- Treatment Protocol Covid-19Document4 pagesTreatment Protocol Covid-19Shiv singhNo ratings yet
- Case PresentationDocument13 pagesCase PresentationAnto BijuNo ratings yet
- General Principles of Antibiotic TherapyDocument44 pagesGeneral Principles of Antibiotic TherapyFadhly SharimanNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- AIIMS issues new guidelines for treatment of Covid-19 casesDocument7 pagesAIIMS issues new guidelines for treatment of Covid-19 casessenthil kumarNo ratings yet
- Tuberculosis and LeprosyDocument43 pagesTuberculosis and LeprosyDianna RoseNo ratings yet
- COVID-19 Management ProtocolDocument13 pagesCOVID-19 Management ProtocolajiNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Case Icu 1Document40 pagesCase Icu 1Salwa KaramanNo ratings yet
- Lenvatinib/Pembrolizumab vs Lenvatinib/Placebo in First Line HCC: Adverse Events ManagementDocument39 pagesLenvatinib/Pembrolizumab vs Lenvatinib/Placebo in First Line HCC: Adverse Events ManagementFERNANDO BUSTAMANTE MORALESNo ratings yet
- CASE PRESENTATION PneumoniaDocument13 pagesCASE PRESENTATION PneumoniaHari Singh RathoreNo ratings yet
- Case Presentation On Chronic BronchitisDocument20 pagesCase Presentation On Chronic BronchitisSafoora RafeeqNo ratings yet
- Anaesthesia For Ect March 2020Document120 pagesAnaesthesia For Ect March 2020Sangkaran KumarNo ratings yet
- Upadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHDocument47 pagesUpadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHNusrat JahanNo ratings yet
- PHC 550 Case-Based Learning 1Document24 pagesPHC 550 Case-Based Learning 1Atiqah AzmiNo ratings yet
- AIIMS COVID Algorithm 1.5-1 PDFDocument1 pageAIIMS COVID Algorithm 1.5-1 PDFAnutosh BhaskarNo ratings yet
- Protocol For COVID-Management Updated Version 2.1 - AIIMS 3 May 2021Document63 pagesProtocol For COVID-Management Updated Version 2.1 - AIIMS 3 May 2021Gopireddy Sivakarthik ReddyNo ratings yet
- COVID-19 Protocol KGMU Version 6.0 17-4-21Document34 pagesCOVID-19 Protocol KGMU Version 6.0 17-4-21Kirtivaan MishraNo ratings yet
- Case Presentation On Dengue Fever: Presented byDocument32 pagesCase Presentation On Dengue Fever: Presented byvyshnavi machirajuNo ratings yet
- PEDI PEARLS: Dr. Cortes Guide to Common Pediatric Respiratory IssuesDocument46 pagesPEDI PEARLS: Dr. Cortes Guide to Common Pediatric Respiratory Issuesthomasfx10100% (1)
- INTERIM CLINICAL GUIDANCE FOR MANAGEMENT OF COVID-19Document1 pageINTERIM CLINICAL GUIDANCE FOR MANAGEMENT OF COVID-19mbhangaleNo ratings yet
- ConnectorDocument4 pagesConnectoryetaung8No ratings yet
- MX Protocol Book FinalDocument42 pagesMX Protocol Book FinalPawan ChoudharyNo ratings yet
- House Call SepsisDocument23 pagesHouse Call SepsisZayar HmunNo ratings yet
- Dobutamine Stress Echocardiography (DSE) GuideDocument11 pagesDobutamine Stress Echocardiography (DSE) GuideNina Rizky FebrianaNo ratings yet
- Acute Exacerbation of COPDDocument14 pagesAcute Exacerbation of COPDMohammad AliNo ratings yet
- Traumatic Brain Injury 2023Document17 pagesTraumatic Brain Injury 2023Fernando Martinez AguilarNo ratings yet
- Crohns DiseaseDocument21 pagesCrohns DiseaseKasuganti koteshwar raoNo ratings yet
- Fundamentals of NursingDocument13 pagesFundamentals of NursingGiselle Chloe Baluya icoNo ratings yet
- MR Muh. Arafah TB (Autosaved)Document14 pagesMR Muh. Arafah TB (Autosaved)tiarapolarisiriuzNo ratings yet
- CovidDocument31 pagesCovidShaheen SultanNo ratings yet
- AIIMS COVID Algorithm Ver 2.0Document1 pageAIIMS COVID Algorithm Ver 2.0jimjose antonyNo ratings yet
- SOP COVID ManagementDocument10 pagesSOP COVID ManagementJerryNo ratings yet
- 2-Shortness of Breath by Dr.hananDocument49 pages2-Shortness of Breath by Dr.hananSoon SheedNo ratings yet
- Respiratory Tract Infections - Med DidacticsDocument59 pagesRespiratory Tract Infections - Med Didacticsapi-649060644No ratings yet
- Shortness of Breath Causes and TreatmentDocument49 pagesShortness of Breath Causes and TreatmentMetkaNo ratings yet
- BPaL L Webinar (002) - 231128 - 174942Document27 pagesBPaL L Webinar (002) - 231128 - 174942AkshayKumarSinghNo ratings yet
- COVID-19 Treatment GuidelinesDocument26 pagesCOVID-19 Treatment GuidelinesStonefalconNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Case Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerDocument19 pagesCase Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerUmme habeebaNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmaprincesszahra6498No ratings yet
- COVID-19 Infection in Children GuideDocument12 pagesCOVID-19 Infection in Children GuideSutirtha RoyNo ratings yet
- AAN Neuromuscular and SCI TalkDocument36 pagesAAN Neuromuscular and SCI TalkEvelina ȘabanovNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- Pediatric Sepsis Topic DiscussionDocument5 pagesPediatric Sepsis Topic Discussionapi-602288180No ratings yet
- Poisoning II FinalDocument45 pagesPoisoning II FinalBi PinNo ratings yet
- WB COVID19 Latest Treatment ProtocolDocument1 pageWB COVID19 Latest Treatment ProtocolRahul AwasthiNo ratings yet
- Respiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkDocument34 pagesRespiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkThea BerteaNo ratings yet
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic Fevernikhil00007100% (1)
- QR Dengue Infection PDF Final PDFDocument8 pagesQR Dengue Infection PDF Final PDFina2407jrNo ratings yet
- REMEDIOS TRINIDAD ROMULADEZ MEDICAL FOUNDATION INC. COLLEGE OF NURSINGDocument4 pagesREMEDIOS TRINIDAD ROMULADEZ MEDICAL FOUNDATION INC. COLLEGE OF NURSINGJamelyn AsuncionNo ratings yet
- Professor Emma BakerDocument23 pagesProfessor Emma BakerNagla FathiNo ratings yet
- Pedia Census ArrythmiaDocument48 pagesPedia Census ArrythmiaBhi-An BatobalonosNo ratings yet
- COVID-19 Quick Reference Guide for Drugs & TreatmentDocument1 pageCOVID-19 Quick Reference Guide for Drugs & TreatmentBoules AtefNo ratings yet
- Vincent Brody Care PlanDocument10 pagesVincent Brody Care PlanKarina Rodriguez50% (2)
- IIM Kashipur EMBA (Analytics) ProgramDocument32 pagesIIM Kashipur EMBA (Analytics) Programmanu_shuklaNo ratings yet
- CV of Arpita Majumder JanaDocument2 pagesCV of Arpita Majumder JanaSujoyDeNo ratings yet
- KolkataDocument1 pageKolkataSujoyDeNo ratings yet
- West Bengal Housing Board (Estd. Under Wb. Act Xxxii of 1972) "Abasan" 105, S.N. BANERJEE ROAD, KOLKATA-700014Document2 pagesWest Bengal Housing Board (Estd. Under Wb. Act Xxxii of 1972) "Abasan" 105, S.N. BANERJEE ROAD, KOLKATA-700014SujoyDeNo ratings yet
- Name:: TH TH TH TH TH NDDocument5 pagesName:: TH TH TH TH TH NDSujoyDeNo ratings yet
- ELECTRICALDocument42 pagesELECTRICALJothimanikkam SomasundaramNo ratings yet
- PKS Brief CVDocument1 pagePKS Brief CVSujoyDeNo ratings yet
- Traffic Notification For One Way Restriction in Kolkata CityDocument10 pagesTraffic Notification For One Way Restriction in Kolkata CitySujoyDeNo ratings yet
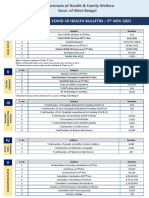
- West Bengal Covid-19 Health Bulletin - 5 NOV 2021 IDocument6 pagesWest Bengal Covid-19 Health Bulletin - 5 NOV 2021 Iyolan daaNo ratings yet
- WB DHFW Bulletin 24TH OCT REPORT FINALDocument6 pagesWB DHFW Bulletin 24TH OCT REPORT FINALSujoyDeNo ratings yet
- WB DHFW Bulletin 24TH OCT REPORT FINALDocument6 pagesWB DHFW Bulletin 24TH OCT REPORT FINALSujoyDeNo ratings yet
- Total Laparo Hysterectomy TLHDocument4 pagesTotal Laparo Hysterectomy TLHSujoyDeNo ratings yet
- KolkataDocument1 pageKolkataSujoyDeNo ratings yet
- Notification 2 For Physical Verification 2021Document9 pagesNotification 2 For Physical Verification 2021SujoyDeNo ratings yet
- DR Sayantan Ganguly: S.ganguly@uu - NLDocument13 pagesDR Sayantan Ganguly: S.ganguly@uu - NLSujoyDeNo ratings yet
- Self-Declaration / Undertaking by Students/Research Scholar/Project JRF Returning To IIT (ISM), DhanbadDocument2 pagesSelf-Declaration / Undertaking by Students/Research Scholar/Project JRF Returning To IIT (ISM), DhanbadSujoyDeNo ratings yet
- Medical Certificate PDFDocument1 pageMedical Certificate PDFFAIQNo ratings yet
- CFD Analysis of Flow in Pump Sump and Physical Validation For Better Performance of PumpDocument7 pagesCFD Analysis of Flow in Pump Sump and Physical Validation For Better Performance of PumpSujoyDeNo ratings yet
- 10th Bry-Air Awards STUDENTS Application Form 14-16Document8 pages10th Bry-Air Awards STUDENTS Application Form 14-16Shivendu AnandNo ratings yet
- ME8T3DDocument3 pagesME8T3DSujoyDeNo ratings yet
- FDGSKG KGLSG S L Lgkslgksks PDocument1 pageFDGSKG KGLSG S L Lgkslgksks PSujoyDeNo ratings yet
- At The Crossroads of Gout and Psoriatic Arthritis: "Psout"Document9 pagesAt The Crossroads of Gout and Psoriatic Arthritis: "Psout"ireneardianiNo ratings yet
- S 1-MathDocument84 pagesS 1-MathREMO MosesNo ratings yet
- Bedside Evaluation of DysphagiaDocument41 pagesBedside Evaluation of Dysphagiaaleeza nomanNo ratings yet
- Drug-Study-Tramadol RyreyDocument3 pagesDrug-Study-Tramadol RyreyJanelle Cabida SupnadNo ratings yet
- USA Today - Vol. 39 No. 255 (14 Sep 2021)Document24 pagesUSA Today - Vol. 39 No. 255 (14 Sep 2021)Xplosion01No ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- Pgi Manimtim - PFC MatrixDocument14 pagesPgi Manimtim - PFC MatrixKim Adarem Joy Manimtim100% (2)
- Bacterial vs Animal Cell ComparisonDocument9 pagesBacterial vs Animal Cell ComparisonMitzi CarreonNo ratings yet
- Pre-Placement Assessment Form - Jan 2023Document4 pagesPre-Placement Assessment Form - Jan 2023Nicole KhouryNo ratings yet
- Exam MCQ عين شمس + AnswersDocument118 pagesExam MCQ عين شمس + AnswersIsmail Ahmed0% (1)
- MCN RLE Sitz Bath Procedure ChecklistDocument3 pagesMCN RLE Sitz Bath Procedure ChecklistHannah Angelu Cabading100% (1)
- SplenectomyDocument17 pagesSplenectomyDONALD UNASHENo ratings yet
- LoperamideDocument1 pageLoperamidekimglaidyl bontuyanNo ratings yet
- Microbiology Lab (Midterms) : November 2015 Dr. Mark CalbanDocument3 pagesMicrobiology Lab (Midterms) : November 2015 Dr. Mark Calbanrichmarkconag1No ratings yet
- Air SanitationDocument8 pagesAir SanitationVignesh ReddyNo ratings yet
- Limb Length DiscrepencyDocument76 pagesLimb Length Discrepencyshan1009No ratings yet
- Lebanon Exams Mrcs Part A Sample QuestionsDocument6 pagesLebanon Exams Mrcs Part A Sample QuestionsNadir AlhussienyNo ratings yet
- Monitoring An IV Site and InfusionDocument4 pagesMonitoring An IV Site and InfusionAlex Cacayan CortinaNo ratings yet
- Taenia Solium Cysticercosis - The Lessons of HistoryDocument4 pagesTaenia Solium Cysticercosis - The Lessons of HistoryAntonio Márquez LaraNo ratings yet
- Anatomy, Abdomen and Pelvis, Female External Genitalia - StatPearls - NCBI BookshelfDocument1 pageAnatomy, Abdomen and Pelvis, Female External Genitalia - StatPearls - NCBI Bookshelfpapoy123100% (1)
- Disturbances in DigestionDocument2 pagesDisturbances in DigestionAnabelle RicoNo ratings yet
- 22 Gait DisordersDocument13 pages22 Gait DisordersAbhilekh SrivastavaNo ratings yet
- ULCERATIVE COLITIS-doneDocument6 pagesULCERATIVE COLITIS-donecory kurdapyaNo ratings yet
- Draft List of MicroorganismsDocument36 pagesDraft List of MicroorganismsAngadNo ratings yet
- Top 100 Pathology Secrets List W/ NotesDocument6 pagesTop 100 Pathology Secrets List W/ NotesPA2014100% (4)
- Pfizer Adverse Event Report - Godspeed Everyone, GDocument22 pagesPfizer Adverse Event Report - Godspeed Everyone, GChristopher CavallaroNo ratings yet
- Fsc-II All EssaysDocument52 pagesFsc-II All EssaysAnas Ahmad100% (2)
- Teaching Students With Autism Spectrum Disorder - Journal MalloryDocument36 pagesTeaching Students With Autism Spectrum Disorder - Journal Malloryapi-5215405080% (1)
- Ed Approach To Foreign BodyDocument42 pagesEd Approach To Foreign BodyAlex MatthewNo ratings yet
- Common Health Problems in ChildrenDocument5 pagesCommon Health Problems in ChildrenLezrae Chescka Javier IlumbaNo ratings yet