You might also like
- Head and Neck Muscle IdentificationDocument3 pagesHead and Neck Muscle IdentificationPrincess Faniega SugatonNo ratings yet
- 2021 Book MusculoskeletalDiseases2021-20Document289 pages2021 Book MusculoskeletalDiseases2021-20Pris Jarrín MD100% (2)
- Trigger Finger and Ganglion Cyct - Seminar Ortho Year 5Document63 pagesTrigger Finger and Ganglion Cyct - Seminar Ortho Year 5Sh Zahra100% (1)
- Wrist and Finger SeminarDocument40 pagesWrist and Finger SeminarMisoNo ratings yet
- Dr. Ajit K VarmaDocument36 pagesDr. Ajit K VarmaDevana MaelissaNo ratings yet
- SCH in PediaDocument58 pagesSCH in PediaSuniel MaheshwariNo ratings yet
- Forearm, Wrist and HandDocument19 pagesForearm, Wrist and HandFloriza de LeonNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Office Orthopaedics: Ramirez, Bryan Paul GDocument57 pagesOffice Orthopaedics: Ramirez, Bryan Paul GBryan Paul RamirezNo ratings yet
- الفصل الثاني محاضرات PDFDocument20 pagesالفصل الثاني محاضرات PDFAZOZ 19No ratings yet
- Facture/Dislocation: R I C EDocument23 pagesFacture/Dislocation: R I C EKrishnamurti KambleNo ratings yet
- Notes On Acute Extensor Tendon InjuryDocument45 pagesNotes On Acute Extensor Tendon InjuryDr.Zahida AkhtarNo ratings yet
- Peripheral Nerve Injury in Upper LimbDocument29 pagesPeripheral Nerve Injury in Upper Limbvenkata ramakrishnaiahNo ratings yet
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocument59 pagesWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNo ratings yet
- Ankylosing Spondylitis 1Document31 pagesAnkylosing Spondylitis 1Salman KhanNo ratings yet
- Musculoskeletal Examination Under GraduatesDocument98 pagesMusculoskeletal Examination Under GraduatesEsraa SalemNo ratings yet
- De Quervain's Tenosynovitis: Dr. Jatin JR3 Year Orthopaed Ics Fmhs Under SGT UniversityDocument31 pagesDe Quervain's Tenosynovitis: Dr. Jatin JR3 Year Orthopaed Ics Fmhs Under SGT UniversityKuldeep PindariaNo ratings yet
- Treating WristDocument71 pagesTreating WristSyahriadin SyamNo ratings yet
- Wrist DropDocument38 pagesWrist DropFardan AnsarNo ratings yet
- First Aid Presentation-Hard and Soft Tissue InjuriesDocument21 pagesFirst Aid Presentation-Hard and Soft Tissue InjuriesKellie GuestNo ratings yet
- Colles' FractureDocument16 pagesColles' FracturePooja ShrivastavNo ratings yet
- Accessory NavicularDocument24 pagesAccessory NavicularsprapurNo ratings yet
- Club Hand RibkaDocument31 pagesClub Hand RibkaRibka TheodoraNo ratings yet
- Musculoskeletal Pain Syndromes ExplainedDocument50 pagesMusculoskeletal Pain Syndromes ExplainedIkhsan Amadea9969No ratings yet
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- SHOULDER AND ELBOW ORTHOPEDICSDocument52 pagesSHOULDER AND ELBOW ORTHOPEDICSmukhtar abddi100% (1)
- Distal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemDocument48 pagesDistal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemNicholas DelaliNo ratings yet
- Orthopaedic Emergencies AndreDocument49 pagesOrthopaedic Emergencies AndreLusi MunawarohNo ratings yet
- nullDocument4 pagesnullرافت العواضيNo ratings yet
- Hand Deformity in Rheumatoid Arthritis: DR Sushil Sharma First Year Orthopedic ResidentDocument38 pagesHand Deformity in Rheumatoid Arthritis: DR Sushil Sharma First Year Orthopedic ResidentSamNo ratings yet
- Meniscal TearDocument6 pagesMeniscal TearAdrian Diago TevesNo ratings yet
- Nur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin PalembangDocument38 pagesNur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin Palembangsoleha09la solehaNo ratings yet
- S T O P: Ports Rauma and Veruse ReventionDocument37 pagesS T O P: Ports Rauma and Veruse ReventionNabiha AjmalNo ratings yet
- Rotator Cuff InjuriesDocument26 pagesRotator Cuff Injuriesanname_girlNo ratings yet
- Flexor Tendon Injury: Dr. BestinDocument53 pagesFlexor Tendon Injury: Dr. Bestinbestin athappilly100% (1)
- Basic Fracture ManagementDocument107 pagesBasic Fracture ManagementPrabath ChinthakaNo ratings yet
- Bedah 2Document226 pagesBedah 2trihanggara mahayasaNo ratings yet
- Colle's FractureDocument7 pagesColle's FracturemadheswariNo ratings yet
- 68 DISEASES 2nd Semsester 3rd Year 1 PDFDocument117 pages68 DISEASES 2nd Semsester 3rd Year 1 PDFJimlord GarciaNo ratings yet
- Scaphoid Fracture, Bennett'S Fracture, Metacarpels, Phalanges FractureDocument61 pagesScaphoid Fracture, Bennett'S Fracture, Metacarpels, Phalanges FracturesenthilNo ratings yet
- ElbowDocument52 pagesElbowAbdallah Samir Mostafa٢٠١٩٠٢١٥٩No ratings yet
- Hand & WristDocument56 pagesHand & WristAbdallah Samir Mostafa٢٠١٩٠٢١٥٩No ratings yet
- Carpal Tunnel Syndrome-AbiDocument34 pagesCarpal Tunnel Syndrome-AbiSri MahadhanaNo ratings yet
- Clavicle (: Result From Falls or A Direct Blow To She Shoulder. CLOSED REDUCTION and ImmobilizationDocument20 pagesClavicle (: Result From Falls or A Direct Blow To She Shoulder. CLOSED REDUCTION and ImmobilizationFreisan ChenNo ratings yet
- (Peserta) Bedah 2 - Mantap Februari 2017Document211 pages(Peserta) Bedah 2 - Mantap Februari 2017karno0% (1)
- Colles Fracture & Knee DislocationDocument38 pagesColles Fracture & Knee DislocationNap91No ratings yet
- RheumatoidDocument35 pagesRheumatoidDeva LekshmiNo ratings yet
- Peripheral Nerve Disorders (Dr. Ken)Document72 pagesPeripheral Nerve Disorders (Dr. Ken)Nurindha Shimelia M ZNo ratings yet
- Injuries Around The ShoulderDocument81 pagesInjuries Around The ShoulderMisoNo ratings yet
- Hand and Wrist ExamDocument80 pagesHand and Wrist ExamxpcoolzNo ratings yet
- Femur Shaft FractureDocument33 pagesFemur Shaft FractureAkash KoulNo ratings yet
- Compressive Neuropathy of Upper LimbDocument49 pagesCompressive Neuropathy of Upper LimbYamunaVaaneeSivalingamNo ratings yet
- Examination of Hand & Common Hand InjuriesDocument165 pagesExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- 4 Shoulder JointDocument50 pages4 Shoulder Jointq77gkyhzs4No ratings yet
- Hand and Wrist Examination GuideDocument49 pagesHand and Wrist Examination GuideAzmi FarhadiNo ratings yet
- Test biceps reflex by tapping the biceps tendon with reflex hammer while arm is supinated.- C6 – Brachioradialis reflexDocument74 pagesTest biceps reflex by tapping the biceps tendon with reflex hammer while arm is supinated.- C6 – Brachioradialis reflexBushra EjazNo ratings yet
- Relieve Numbness & Tingling with Ulnar Nerve Entrapment TreatmentDocument19 pagesRelieve Numbness & Tingling with Ulnar Nerve Entrapment TreatmentChristian SolihinNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Biomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KDocument46 pagesBiomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KGio BalisiNo ratings yet
- Referat Claw and Club Hand: Ribka Theodora - Hand 3 Mentor: Dr. Betha Egih Riestiano, Spbp-ReDocument25 pagesReferat Claw and Club Hand: Ribka Theodora - Hand 3 Mentor: Dr. Betha Egih Riestiano, Spbp-ReRibka TheodoraNo ratings yet
- Patient Preferences in Knee Prostheses: J. W. PritchettDocument4 pagesPatient Preferences in Knee Prostheses: J. W. PritchettDave R. SilverNo ratings yet
- Core Stix Instructional RoutinesDocument11 pagesCore Stix Instructional RoutinesAmber Riley100% (1)
- Jin Goo Kim - Knee Arthroscopy - An Up-to-Date Guide-Springer (2021)Document370 pagesJin Goo Kim - Knee Arthroscopy - An Up-to-Date Guide-Springer (2021)Fernando FernandezNo ratings yet
- Sigma CR150 Surgical TechniqueDocument54 pagesSigma CR150 Surgical Techniquegeorgiana.brinza67% (3)
- Anatomy (Patellofemoral Joint)Document3 pagesAnatomy (Patellofemoral Joint)Andy Delos ReyesNo ratings yet
- Anatomical-Positions-Directional-Terms PE 2 ACTIVITY - FLORES, RENNETH READocument9 pagesAnatomical-Positions-Directional-Terms PE 2 ACTIVITY - FLORES, RENNETH REARenneth Rea FloresNo ratings yet
- Musculoskeletal Curriculum: History & Physical Exam of The ShoulderDocument60 pagesMusculoskeletal Curriculum: History & Physical Exam of The Shoulderhis.thunder122100% (1)
- Type of Joints: Group MembersDocument21 pagesType of Joints: Group MembersBeni Ram RawalNo ratings yet
- Video A KinesiologiDocument16 pagesVideo A KinesiologiDicky Christa KurniawanNo ratings yet
- A Practical Guide For Performing Arthrography Under Fluoroscopic or Ultrasound GuidanceDocument10 pagesA Practical Guide For Performing Arthrography Under Fluoroscopic or Ultrasound GuidanceSnehanshNo ratings yet
- Effect of Hamstring Emphasized Resistance Training On H-Q Strength RatioDocument7 pagesEffect of Hamstring Emphasized Resistance Training On H-Q Strength RatioRaja Nurul JannatNo ratings yet
- Built by Science PDFDocument73 pagesBuilt by Science PDFHeidi Y. Matos GaliciaNo ratings yet
- Shoulder - Rotator Cuff - Arthroscopic Rotator Cuff Repair Medium To Large Tears (Type II) PDFDocument4 pagesShoulder - Rotator Cuff - Arthroscopic Rotator Cuff Repair Medium To Large Tears (Type II) PDFAndresLeivaMckendrickNo ratings yet
- Anatomy MS WristJointSGDDocument24 pagesAnatomy MS WristJointSGDSpencerNo ratings yet
- Pathway For Shoulder PainDocument1 pagePathway For Shoulder Painrizk86No ratings yet
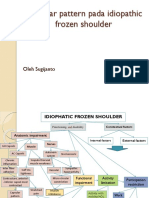
- Capsular pattern identification in idiopathic frozen shoulderDocument11 pagesCapsular pattern identification in idiopathic frozen shoulderRhany JulyatiNo ratings yet
- Joints Movement Powerpoint PDFDocument21 pagesJoints Movement Powerpoint PDFDean Albert Arnejo100% (1)
- Treatment and Rehabilitation of Fractures (Stanley Hoppenfeld)Document1 pageTreatment and Rehabilitation of Fractures (Stanley Hoppenfeld)小蓮花No ratings yet
- 01 Basics in Manual TherapyDocument74 pages01 Basics in Manual TherapynoorNo ratings yet
- Fix Your Caveman Posture in 4 PartsDocument87 pagesFix Your Caveman Posture in 4 PartsaskofsublimeNo ratings yet
- Dirkwinkel Johanna Sophie Mefst 2017 Diplo SveucDocument59 pagesDirkwinkel Johanna Sophie Mefst 2017 Diplo SveucJulenda CintarinovaNo ratings yet
- Kode ICD Orthopedi 2 2022Document8 pagesKode ICD Orthopedi 2 2022dian putri yulianiNo ratings yet
- Joint DislocationDocument30 pagesJoint DislocationamriNo ratings yet
- Distal Radius and UlnaDocument40 pagesDistal Radius and UlnaDia CembranoNo ratings yet
- The Effect of Open and Closed Chain Exercise and Knee Joint Position On Patellar Tracking in Lateral Patellar Compression SyndromeDocument7 pagesThe Effect of Open and Closed Chain Exercise and Knee Joint Position On Patellar Tracking in Lateral Patellar Compression SyndromeSalem DaldoulNo ratings yet
- Comparing VMO and Gluteus Medius Strengthening Exercises to Normalize Q Angle in Knee OADocument67 pagesComparing VMO and Gluteus Medius Strengthening Exercises to Normalize Q Angle in Knee OAJigyasa JuyalNo ratings yet