You might also like
- Ketut Suryana Ketut SuardamanaDocument46 pagesKetut Suryana Ketut SuardamanaYogiswara KarangNo ratings yet
- Anaphylaxis Reaction & Drug Allergy 2Document47 pagesAnaphylaxis Reaction & Drug Allergy 2telusurNo ratings yet
- Clinical Manifestation and Management of Anaphylactic ReactionDocument9 pagesClinical Manifestation and Management of Anaphylactic Reactionandi darul aqsaNo ratings yet
- AnaphylaxisDocument34 pagesAnaphylaxisffNo ratings yet
- Anaphylaxis 2Document34 pagesAnaphylaxis 2luckyNo ratings yet
- Anaphylaxis: Allergy, Asthma & Clinical ImmunologyDocument8 pagesAnaphylaxis: Allergy, Asthma & Clinical ImmunologyBabad BagusNo ratings yet
- Anaphylaxis: Anlidya Permatasari GDocument30 pagesAnaphylaxis: Anlidya Permatasari GanlidyaNo ratings yet
- Dr. Az Rifki, Span - Kic Dept. Anestesiologi Dan Reanimasi FK-FKG Univ. Baiturrahmah / Rs Islam Siti Rahmah PadangDocument49 pagesDr. Az Rifki, Span - Kic Dept. Anestesiologi Dan Reanimasi FK-FKG Univ. Baiturrahmah / Rs Islam Siti Rahmah PadangDewi Arimbi PratamaNo ratings yet
- Anaphylaxis: DR - Arvinth SoundarrajanDocument26 pagesAnaphylaxis: DR - Arvinth SoundarrajanP Vinod KumarNo ratings yet
- Anaphylaxis ArticuloDocument12 pagesAnaphylaxis ArticuloFrancelia Quiñonez RuvalcabaNo ratings yet
- Anaphylaxis: Review Open AccessDocument7 pagesAnaphylaxis: Review Open AccessRadyaAgriNo ratings yet
- Anaphylaxis ReactionDocument27 pagesAnaphylaxis ReactiongusriaNo ratings yet
- Anaphylaxis TADocument54 pagesAnaphylaxis TAUriko ZoeNo ratings yet
- Allergy Overview: - Nomenclature - Pathophysiology - Diagnosis - ManagementDocument96 pagesAllergy Overview: - Nomenclature - Pathophysiology - Diagnosis - ManagementPhaimNo ratings yet
- Anaphylaxis: Diagnosis, Treatment and PreventionDocument48 pagesAnaphylaxis: Diagnosis, Treatment and PreventionLuthfita RahmawatiNo ratings yet
- Anaphylaxis: Diagnosis and Management: Mja Practice Essentials - AllergyDocument7 pagesAnaphylaxis: Diagnosis and Management: Mja Practice Essentials - AllergyFran ramos ortegaNo ratings yet
- Internal Medicine 0604B ANAPHYLAXISDocument6 pagesInternal Medicine 0604B ANAPHYLAXISSiselle FajardoNo ratings yet
- Allergy: Drug Reaction ClassificationDocument6 pagesAllergy: Drug Reaction ClassificationMatthieu FortinNo ratings yet
- Reaksi Anafilaksis: DR - Wisda Widiastuti, SPPD FK Universitas BaiturrahmahDocument26 pagesReaksi Anafilaksis: DR - Wisda Widiastuti, SPPD FK Universitas BaiturrahmahWulan afriNo ratings yet
- Management Syok Anafilaktik UnbrahDocument31 pagesManagement Syok Anafilaktik UnbrahSasha ManoNo ratings yet
- Anaphylactic Shock Signs, Symptoms, TreatmentDocument29 pagesAnaphylactic Shock Signs, Symptoms, TreatmentHIND100% (7)
- Anaphylaxis: Diagnosis and Management: The Medical Journal of Australia October 2006Document8 pagesAnaphylaxis: Diagnosis and Management: The Medical Journal of Australia October 2006DidiNo ratings yet
- Anaphylaxis Diagnosis and ManagementDocument10 pagesAnaphylaxis Diagnosis and Managementd dNo ratings yet
- Anaphylaxis ReactionDocument27 pagesAnaphylaxis Reactionmau tauNo ratings yet
- Anaphylaxis Reaction: Marshell Tendean, MD, DPCP Department of Internal Medicine UKRIDA, JakartaDocument27 pagesAnaphylaxis Reaction: Marshell Tendean, MD, DPCP Department of Internal Medicine UKRIDA, JakartaJessiNo ratings yet
- Anaphylaxis Update: Be Prepared!: Ari R Cohen, MD, FAAP Massachusetts General Hospital Boston, MADocument45 pagesAnaphylaxis Update: Be Prepared!: Ari R Cohen, MD, FAAP Massachusetts General Hospital Boston, MAAsfiksia NeonatorumNo ratings yet
- University of the Philippines Manila College of Nursing Drug StudyDocument3 pagesUniversity of the Philippines Manila College of Nursing Drug StudyAna Luisa Conejos ConeseNo ratings yet
- Reaksi AnafilaksisDocument34 pagesReaksi AnafilaksisPutri Reno IntanNo ratings yet
- Immunopathology QuestionsDocument123 pagesImmunopathology QuestionsNaeman GoetzNo ratings yet
- BJA 2019 - Allergic Conditions and Perioperative SettingDocument17 pagesBJA 2019 - Allergic Conditions and Perioperative SettingMILTON HALYSONNo ratings yet
- Anaphylaxis Copy1Document22 pagesAnaphylaxis Copy1MunishNo ratings yet
- Managing Anaphylactic Shock & Laryngeal EdemaDocument9 pagesManaging Anaphylactic Shock & Laryngeal EdemaAyu AnnisaNo ratings yet
- AnafilaksisDocument27 pagesAnafilaksisAhmad ZakiNo ratings yet
- Alsangedy Bullets For Paces: AcromegalyDocument20 pagesAlsangedy Bullets For Paces: AcromegalyIgor BatistaNo ratings yet
- Clin Immunology Lecture 3 For DentistsDocument97 pagesClin Immunology Lecture 3 For Dentistsnaveenyadav7857No ratings yet
- Alergi, Pseudoalergi, Rhematoid Arthritis, GhoutDocument39 pagesAlergi, Pseudoalergi, Rhematoid Arthritis, GhoutMaresa HananielNo ratings yet
- By Mayo Clinic StaffDocument5 pagesBy Mayo Clinic StaffTry Febriani SiregarNo ratings yet
- KULIAH Anaphylaxis - 0408 2Document65 pagesKULIAH Anaphylaxis - 0408 2AudioBhaskara TitalessyNo ratings yet
- RTM 5Document7 pagesRTM 5Christine Danica BiteraNo ratings yet
- Anafilaksis PDFDocument27 pagesAnafilaksis PDFAvicenna_MSC100% (1)
- Urticaria and AngioedemaDocument54 pagesUrticaria and AngioedemaSRIRAM CKNo ratings yet
- Antiallergic Drugs, Drugs For Immune SistemDocument38 pagesAntiallergic Drugs, Drugs For Immune SistemTawhid ZihadNo ratings yet
- Web 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyDocument38 pagesWeb 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyEdzhar HasiholanNo ratings yet
- Reaksi AnafilaktikDocument34 pagesReaksi AnafilaktikOlla AndraNo ratings yet
- AnaphylaxisDocument60 pagesAnaphylaxisRazia JafferyNo ratings yet
- Patofis 9 Alergi, Pseudoalergi, Rhematoid Arthritis, Ghout - NEWDocument42 pagesPatofis 9 Alergi, Pseudoalergi, Rhematoid Arthritis, Ghout - NEWDea NaswaniyahNo ratings yet
- Steroid in EntDocument113 pagesSteroid in Entdrazmy2006100% (1)
- Dönem 5 Ingilizce 02.04Document53 pagesDönem 5 Ingilizce 02.04Sarper Hikmet TAZENo ratings yet
- Urticaria and AngioedemaDocument20 pagesUrticaria and AngioedemaAhmad KusayiriNo ratings yet
- Anaphylactic Death FinalDocument73 pagesAnaphylactic Death Finalkhaled eissaNo ratings yet
- Guillain Barre SyndromeDocument43 pagesGuillain Barre Syndromegabrielle magdaraogNo ratings yet
- AnaphylaxisDocument16 pagesAnaphylaxisEdgarNo ratings yet
- 44 - AnaphylaxisDocument16 pages44 - AnaphylaxisWillean Quispe QueaNo ratings yet
- Shock AnaphylaticDocument15 pagesShock AnaphylaticAvif PutraNo ratings yet
- DRUG ALLERGY GUIDEDocument61 pagesDRUG ALLERGY GUIDEadysti100% (1)
- Pediatric AnaphylaxisDocument19 pagesPediatric AnaphylaxisancillaagraynNo ratings yet
- AnaphylaxisDocument5 pagesAnaphylaxisTam Kan SayımıNo ratings yet
- Managing Anaphylactic Shock Journal of Modern Pharmacy 2006Document3 pagesManaging Anaphylactic Shock Journal of Modern Pharmacy 2006Saputro AbdiNo ratings yet
- Kgday New Mistake Try EverythingDocument11 pagesKgday New Mistake Try EverythingBunda OlifiaNo ratings yet
- Lecture 1 - Respiratory System Baru 2Document56 pagesLecture 1 - Respiratory System Baru 2Pande Putu Rangga RadityaNo ratings yet
- Presentation Number OneDocument6 pagesPresentation Number OneArtawa Darma YudaNo ratings yet
- (Kuliah 1) PROFESIONALISME KEDOKTERAN 2012Document14 pages(Kuliah 1) PROFESIONALISME KEDOKTERAN 2012Artawa Darma YudaNo ratings yet
- Anemia Defisiensi Besi 2013Document27 pagesAnemia Defisiensi Besi 2013Artawa Darma YudaNo ratings yet
- (KULIAH 10) Motility 2kul2011Document38 pages(KULIAH 10) Motility 2kul2011Artawa Darma YudaNo ratings yet
- Dry Eye Syndrome PPPDocument44 pagesDry Eye Syndrome PPPHendra GunawanNo ratings yet
- Lesi Prakanker Dan Tumor GinekologiDocument98 pagesLesi Prakanker Dan Tumor GinekologiArtawa Darma YudaNo ratings yet
- Definisi - : Susilawathi Et Al. BMC Infectious Diseases 2012Document1 pageDefinisi - : Susilawathi Et Al. BMC Infectious Diseases 2012Artawa Darma YudaNo ratings yet
- Definisi - : Susilawathi Et Al. BMC Infectious Diseases 2012Document1 pageDefinisi - : Susilawathi Et Al. BMC Infectious Diseases 2012Artawa Darma YudaNo ratings yet
- Jurnal Rabies InggrisDocument5 pagesJurnal Rabies InggrisArtawa Darma YudaNo ratings yet
- 04 10 14 Embriology IDocument6 pages04 10 14 Embriology IArtawa Darma YudaNo ratings yet
- Peritonsillar AbsesDocument4 pagesPeritonsillar AbsesArtawa Darma YudaNo ratings yet
- LiteraturDocument1 pageLiteraturArtawa Darma YudaNo ratings yet
- Chapter 8 Practice 1Document19 pagesChapter 8 Practice 1pallavikvs27No ratings yet
- Chapter 17 - Laboratory Testing and Diagnostics - APIC Text OnlineDocument10 pagesChapter 17 - Laboratory Testing and Diagnostics - APIC Text OnlineManalAbdelazizNo ratings yet
- Sexually Transmitted DiseasesDocument5 pagesSexually Transmitted Diseasesgodiee77No ratings yet
- EPISCLERITIS & ScleritisDocument14 pagesEPISCLERITIS & ScleritisChikita Artia SariNo ratings yet
- Psychoneuroimmunology: From Philosophy, Intuition, and Folklore To A Recognized ScienceDocument6 pagesPsychoneuroimmunology: From Philosophy, Intuition, and Folklore To A Recognized ScienceMita MiftaNo ratings yet
- About Inflammation and InfectionDocument2 pagesAbout Inflammation and InfectionHAZRULNo ratings yet
- Case Presentation-ChickenpoxDocument41 pagesCase Presentation-ChickenpoxShaliniNo ratings yet
- Report On The Global Statistical Data of COVIDDocument3 pagesReport On The Global Statistical Data of COVIDChristian Angelo G. MontigoNo ratings yet
- HEPATITIS B in The WorkplaceDocument51 pagesHEPATITIS B in The WorkplaceApril Joy MercadoNo ratings yet
- Microbiology at A GlanceDocument126 pagesMicrobiology at A GlanceMuhammad UsmanNo ratings yet
- Pharmacology 2Document26 pagesPharmacology 2Subham SinghNo ratings yet
- COVID-19 Current State Analysis and Forecasting For The DFW RegionDocument14 pagesCOVID-19 Current State Analysis and Forecasting For The DFW RegionSourav SutradharNo ratings yet
- Graft Rejection Ppt1Document14 pagesGraft Rejection Ppt1GEETA MOHAN100% (2)
- Malaria Investigation in Banjarnegara VillageDocument9 pagesMalaria Investigation in Banjarnegara VillagenawangprimailmiafeeNo ratings yet
- Lista DiagnosticeDocument566 pagesLista DiagnosticeGeanina MireaNo ratings yet
- MeningitisDocument15 pagesMeningitisAniket Singh100% (1)
- Autoimmune Bullous Diseases Associations: Suzana Ljubojevic, MD, PHD, Jasna Lipozen Čić, MD, PHDDocument17 pagesAutoimmune Bullous Diseases Associations: Suzana Ljubojevic, MD, PHD, Jasna Lipozen Čić, MD, PHDRunuk BhandariNo ratings yet
- Circulatory System - Blood: Al-Farabi Kazakh National University Higher School of MedicineDocument35 pagesCirculatory System - Blood: Al-Farabi Kazakh National University Higher School of MedicineDevaDharshiniNo ratings yet
- 2 Transplantation ImmunologyDocument33 pages2 Transplantation Immunologykirubel getyeNo ratings yet
- Braun Falco 2012Document7 pagesBraun Falco 2012Alexandra OpreaNo ratings yet
- Multiple Sclerosis PDFDocument1 pageMultiple Sclerosis PDFAcey TfNo ratings yet
- 1.parotitis Practice Essentials, Pathophysiology, EpidemiologyDocument12 pages1.parotitis Practice Essentials, Pathophysiology, Epidemiologyandi elsa mulya pratiwiNo ratings yet
- Prisons and Health, 9 Infectious Diseases in PrisonDocument8 pagesPrisons and Health, 9 Infectious Diseases in PrisonBam ManNo ratings yet
- Salmonella Infections: (Salmonelloses)Document56 pagesSalmonella Infections: (Salmonelloses)andualemNo ratings yet
- Microbiology and Parasitology Week 3. ABCDDocument21 pagesMicrobiology and Parasitology Week 3. ABCDohsehuns wifeuNo ratings yet
- Affimed Presentation-Mar2020 Final-1 PDFDocument22 pagesAffimed Presentation-Mar2020 Final-1 PDFElio GonzalezNo ratings yet
- Autismo y AutoinmunidadDocument50 pagesAutismo y AutoinmunidadPsicoterapia InfantilNo ratings yet
- Somatic RecombinationDocument5 pagesSomatic RecombinationNoor Ul NaeemNo ratings yet
- Annotated BibliographyDocument3 pagesAnnotated BibliographypeterhjeonNo ratings yet
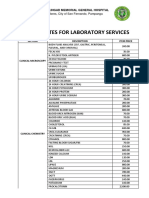
- JBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalDocument4 pagesJBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalApril NNo ratings yet