You might also like
- Episiotomy and RepairDocument20 pagesEpisiotomy and RepairwendeliciousNo ratings yet
- EPISIOTOMYDocument17 pagesEPISIOTOMYKaye Arriane TenorioNo ratings yet
- Episeotomy Procedure, Care, ComplicationsDocument3 pagesEpiseotomy Procedure, Care, ComplicationsNejib M/AminNo ratings yet
- Episiotomy: Dr. Fekadu R (MD) November, 2012/19Document11 pagesEpisiotomy: Dr. Fekadu R (MD) November, 2012/19tareNo ratings yet
- Revisión Histórica de EpisiotomíaDocument7 pagesRevisión Histórica de EpisiotomíaAlvaro OyarceNo ratings yet
- Epi SutureDocument7 pagesEpi SutureyayitsnayNo ratings yet
- 10 1002@micr 30633Document6 pages10 1002@micr 30633carlosNo ratings yet
- Bille Et Al 2019Document5 pagesBille Et Al 2019Walid SasiNo ratings yet
- Zingaretti Et Al. 2019Document5 pagesZingaretti Et Al. 2019Walid SasiNo ratings yet
- Procedure ON: EpisiotomyDocument7 pagesProcedure ON: EpisiotomyShalabh JoharyNo ratings yet
- Government College of Nursing: Procedure ONDocument6 pagesGovernment College of Nursing: Procedure ONpriyanka100% (6)
- Costochondral GraftsDocument5 pagesCostochondral Graftssmartdoc36100% (1)
- Presentation 1Document11 pagesPresentation 1Leo PrabhuNo ratings yet
- 839 1 FullDocument3 pages839 1 FullDiego AndradeNo ratings yet
- Thoracic EmpyemaDocument3 pagesThoracic EmpyemaDiego AndradeNo ratings yet
- Episiotomy DefinitionDocument4 pagesEpisiotomy Definitionnursing school0% (1)
- Episiotomy: By: Charisse Ann G. GasatayaDocument23 pagesEpisiotomy: By: Charisse Ann G. GasatayaCharisse Ann GasatayaNo ratings yet
- EpisiotomyDocument49 pagesEpisiotomyBharat ThapaNo ratings yet
- Episiotomy VideoDocument20 pagesEpisiotomy VideoEkram Gamal MorshedʚɞNo ratings yet
- Direct-To-Implant Breast ReconstructionDocument3 pagesDirect-To-Implant Breast ReconstructionCarlos Javier SolorzaNo ratings yet
- Nur 146 RleDocument47 pagesNur 146 RleKeziah Marie Chua Santa-AnaNo ratings yet
- EpisiotomyDocument30 pagesEpisiotomysubi100% (1)
- EpisiotomyDocument7 pagesEpisiotomyLenny SucalditoNo ratings yet
- Surgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDocument4 pagesSurgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDwarika Prasad BajgaiNo ratings yet
- Internal MastopexyDocument7 pagesInternal MastopexyfumblefumbleNo ratings yet
- Keyhole Vertical Mini-Abdominoplasty For Correction of Lower Abdominal StriaeDocument5 pagesKeyhole Vertical Mini-Abdominoplasty For Correction of Lower Abdominal StriaeAmirNo ratings yet
- Episiotomy RcogDocument1 pageEpisiotomy RcogAisha RizwanNo ratings yet
- Performing and Suturing An EpisiotomyDocument4 pagesPerforming and Suturing An EpisiotomymanjuNo ratings yet
- Facemask Anaesthesia Update 2011 PDFDocument5 pagesFacemask Anaesthesia Update 2011 PDFAhmad Giffar DantoNo ratings yet
- Types of EpisiotomiesDocument2 pagesTypes of EpisiotomieskewpietheresaNo ratings yet
- Unit 9 Episiotomy and Nursing Management: 9.0 ObjectivesDocument8 pagesUnit 9 Episiotomy and Nursing Management: 9.0 ObjectivesSudip Kumar DeyNo ratings yet
- Vaginal Agenesis or HypoplasiaDocument18 pagesVaginal Agenesis or Hypoplasianikd_6No ratings yet
- EpisiotomyDocument30 pagesEpisiotomymob3100% (2)
- Median Sternotomy ProcedureDocument5 pagesMedian Sternotomy ProcedureNelly NehNo ratings yet
- Ecotv PDFDocument18 pagesEcotv PDFmacarena castilloNo ratings yet
- Five Steps To Internal Mammary Vessel Preparation in Less Than 15 MinutesDocument3 pagesFive Steps To Internal Mammary Vessel Preparation in Less Than 15 MinutesGökhan AkçiçekNo ratings yet
- Safe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalDocument4 pagesSafe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalJerahmeel Sombilon GenillaNo ratings yet
- New Fon I-Unit 3 Safety Comfort & Bed MakingDocument84 pagesNew Fon I-Unit 3 Safety Comfort & Bed MakingbarrichabarrichooNo ratings yet
- Delayed Repair of Large Myelomeningoceles: TechnicalnoteDocument3 pagesDelayed Repair of Large Myelomeningoceles: TechnicalnoteTeuku Arie HidayatNo ratings yet
- Scar Endometriosis Case Report With Literature ReviewDocument3 pagesScar Endometriosis Case Report With Literature ReviewelsaNo ratings yet
- EpisiotomyDocument6 pagesEpisiotomyNishaThakuri100% (1)
- NCM 107 SKL FinalsDocument33 pagesNCM 107 SKL FinalsCyriz Ann Mae PacisNo ratings yet
- Lateral Thigh and Anterolateral Thigh Free Tissue Transfer: Background, History of The Procedure, IndicationsDocument12 pagesLateral Thigh and Anterolateral Thigh Free Tissue Transfer: Background, History of The Procedure, IndicationsNaenay WannatrakoolNo ratings yet
- Bolla 2016Document4 pagesBolla 2016kübra özpınarNo ratings yet
- Obstetric Operations and Procedures - CompleteDocument46 pagesObstetric Operations and Procedures - CompleteMax ZealNo ratings yet
- Access Surgery - PrintDocument56 pagesAccess Surgery - PrintJeya SudhaharNo ratings yet
- EpsiotomyDocument2 pagesEpsiotomyJazzlyneNo ratings yet
- The Single Incision Minimally Invasive (SIMI) Neck LiftDocument9 pagesThe Single Incision Minimally Invasive (SIMI) Neck Liftwmaiana90No ratings yet
- Chest Tube InsertionDocument4 pagesChest Tube InsertionElton Dias PinheiroNo ratings yet
- Lejour Reduction MammoplastyDocument6 pagesLejour Reduction MammoplastyMiguelito JohnsonNo ratings yet
- PIIS1043181018300332Document4 pagesPIIS1043181018300332Ottofianus Alvedo Hewick KalangiNo ratings yet
- APPENDECTOMYDocument12 pagesAPPENDECTOMYayouNo ratings yet
- Or AssignmentDocument5 pagesOr AssignmentJohara MacasindelNo ratings yet
- The Big Five-Lifesaving Procedures in The Trauma BayDocument22 pagesThe Big Five-Lifesaving Procedures in The Trauma BayBruce Fredy Chino ChambillaNo ratings yet
- Birth DefectDocument80 pagesBirth DefectGIRUM BELAYNo ratings yet
- Thoracic Empyema: A Jaffé, G Cohen A Role For Primary Video Assisted Thoracoscopic Surgery ?Document3 pagesThoracic Empyema: A Jaffé, G Cohen A Role For Primary Video Assisted Thoracoscopic Surgery ?Hafshah SumayyahNo ratings yet
- Daane 1999Document11 pagesDaane 1999nikitagustiNo ratings yet
- OB2 RLE SAS 6 Versions SAS 7 Caesarian Section SAS 8 Uterine AtonyDocument26 pagesOB2 RLE SAS 6 Versions SAS 7 Caesarian Section SAS 8 Uterine AtonyHana LandinginNo ratings yet
- What Is An Intravenous Pyelogram (IVP) ?: X-Ray Ureters Bladder Contrast MaterialDocument6 pagesWhat Is An Intravenous Pyelogram (IVP) ?: X-Ray Ureters Bladder Contrast MaterialVirgz PalNo ratings yet
- Auditing AssignmentDocument2 pagesAuditing AssignmentJean Aubrey GacayanNo ratings yet
- Evaluation of The Neonate With Seizures 2020Document7 pagesEvaluation of The Neonate With Seizures 2020Eduardo Rios DuboisNo ratings yet
- Helen Rose Cepeda - Activity 1Document2 pagesHelen Rose Cepeda - Activity 1Helen Rose CepedaNo ratings yet
- 1319 Case StudyDocument7 pages1319 Case StudyElizabeth SamudioNo ratings yet
- EVALUATE Match Each Subfield of Psychology With The Issues or Questions Posed BelowDocument2 pagesEVALUATE Match Each Subfield of Psychology With The Issues or Questions Posed BelowAlexandra TorresNo ratings yet
- Neurobiology of The Structure of Personality Dopamine, Facilitation of Incentive Motivation, and Extraversion BEHAVIORAL AND BRAIN SCIENCES (1999) 22Document79 pagesNeurobiology of The Structure of Personality Dopamine, Facilitation of Incentive Motivation, and Extraversion BEHAVIORAL AND BRAIN SCIENCES (1999) 22McArtur100% (1)
- Assignment 3: Consumer LearningDocument4 pagesAssignment 3: Consumer LearninglaibaNo ratings yet
- Vineland Adaptive Behaviour Scales (VABS) - IIDocument6 pagesVineland Adaptive Behaviour Scales (VABS) - IIAlan Marsh67% (3)
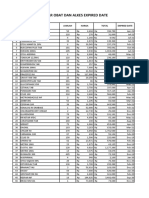
- DAFTAR OBAT ALKES ED RSJHMK UpdateDocument5 pagesDAFTAR OBAT ALKES ED RSJHMK UpdateINSTALASI FARMASI RSJHMKNo ratings yet
- Benchmark Adverse SituationsDocument6 pagesBenchmark Adverse Situationsapi-354423377No ratings yet
- Health and Hygiene ProgrammeDocument21 pagesHealth and Hygiene ProgrammeJNV_DVG50% (8)
- Periodontology: Richard Palmer Peter Floyd EditorsDocument224 pagesPeriodontology: Richard Palmer Peter Floyd EditorsAbdelkhalek BouararaNo ratings yet
- Perioperative NursingDocument8 pagesPerioperative NursinglovethestarNo ratings yet
- Russell-Taylor Delta-Tibial Interlocking Nail TechniqueDocument30 pagesRussell-Taylor Delta-Tibial Interlocking Nail TechniquemikeydamanNo ratings yet
- Health and Remedies Information Gap Activities - 141815Document6 pagesHealth and Remedies Information Gap Activities - 141815Andrés DíazNo ratings yet
- Histological Approach To Nutritional Status of The Liver and Gut in Atlantic Cod Larvae With and Without Bile Salt SupplementationDocument14 pagesHistological Approach To Nutritional Status of The Liver and Gut in Atlantic Cod Larvae With and Without Bile Salt SupplementationJan SzczepaniakNo ratings yet
- The Mysterious Death of Dr. SebiDocument15 pagesThe Mysterious Death of Dr. SebiJason Carter100% (1)
- William Bridges Transitions OverviewDocument2 pagesWilliam Bridges Transitions OverviewReveln Consults67% (3)
- Wound NursingDocument22 pagesWound NursingAgeng Catur WicaksonoNo ratings yet
- M - Medications: Discharge PlanningDocument4 pagesM - Medications: Discharge Planningalynnavictoria100% (4)
- Lost at School: Points To PonderDocument59 pagesLost at School: Points To PonderMeridyth Taylor100% (2)
- Free Powerbuilding Program Ben PollackDocument6 pagesFree Powerbuilding Program Ben PollackTevinWaiguru0% (3)
- Data Base and History: Type of Previous Illness Date Type of Previous Illness DateDocument12 pagesData Base and History: Type of Previous Illness Date Type of Previous Illness DateAngel CañaresNo ratings yet
- Rhetorical Analysis FinalDocument6 pagesRhetorical Analysis Finalapi-500722562No ratings yet
- Tamir Hands of ClitroidectomyDocument5 pagesTamir Hands of ClitroidectomyTechnic RealityNo ratings yet
- Concept Map Mental HealthDocument2 pagesConcept Map Mental HealthRhina FutrellNo ratings yet
- 2.7 AssessmentDocument6 pages2.7 AssessmentVani DeswalNo ratings yet
- Dr. Agussalim Bukhari, M.Med, PH.D, SP - GK (K)Document47 pagesDr. Agussalim Bukhari, M.Med, PH.D, SP - GK (K)Vika LeiwaNo ratings yet
- KetosterilDocument8 pagesKetosterilChristian OrevilloNo ratings yet