You might also like
- Cardiovascular Shunt Imaging FindingsDocument20 pagesCardiovascular Shunt Imaging FindingsRoberto HutapeaNo ratings yet
- Acyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianDocument98 pagesAcyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianVijayakanth VijayakumarNo ratings yet
- Aortic StenosisDocument8 pagesAortic Stenosisdr.moni.co.ukNo ratings yet
- CardiologyDocument62 pagesCardiologysee yinNo ratings yet
- The Heart: Development and Clinical PointsDocument54 pagesThe Heart: Development and Clinical PointsHfm 4No ratings yet
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (4)
- Conventional Radiography in Cardiac Chamber EnlargementDocument71 pagesConventional Radiography in Cardiac Chamber EnlargementDr KhanNo ratings yet
- Cardiac Cycle JVPDocument70 pagesCardiac Cycle JVPAstrid PramudyaaNo ratings yet
- Pathology of HEART - 1Document175 pagesPathology of HEART - 1Abdukadir AzamNo ratings yet
- Wk7 PLP Cardiovascular Disorder Part 1,2,3,4Document210 pagesWk7 PLP Cardiovascular Disorder Part 1,2,3,4claire yowsNo ratings yet
- Cardiac Congenital Disease Types and PresentationsDocument27 pagesCardiac Congenital Disease Types and Presentationsnovitafitri123No ratings yet
- Cardiopatii Congenitale 17-18 enDocument74 pagesCardiopatii Congenitale 17-18 enMatei PopescuNo ratings yet
- Cardiac Anatomy and Physiology ReviewDocument144 pagesCardiac Anatomy and Physiology ReviewNb + XB = AVNo ratings yet
- Congenital Heart Disease ExplainedDocument31 pagesCongenital Heart Disease ExplainedAlvienz SaputraNo ratings yet
- Cvs2-k1 (Jp-pjb Pada Dewasa)Document81 pagesCvs2-k1 (Jp-pjb Pada Dewasa)32 sebastian Josia N.No ratings yet
- The Human Heart and Circulatory System: An OverviewDocument36 pagesThe Human Heart and Circulatory System: An OverviewLindiwe GoweNo ratings yet
- Congenital Heart Disease: Patent Ductus ArteriosusDocument43 pagesCongenital Heart Disease: Patent Ductus ArteriosusanandafirstyNo ratings yet
- Understand Basic Cardiac Structure and FunctionDocument13 pagesUnderstand Basic Cardiac Structure and FunctiondeaNo ratings yet
- 1.01 Development of The CVSDocument24 pages1.01 Development of The CVSJedoNo ratings yet
- Valvular DiseasesDocument45 pagesValvular DiseasesKen WayNo ratings yet
- Congenital Heart DiseaseDocument38 pagesCongenital Heart DiseaseSnIP StandredNo ratings yet
- Cardiology Course Outline on Functional Anatomy and PhysiologyDocument19 pagesCardiology Course Outline on Functional Anatomy and PhysiologyImraan MohaNo ratings yet
- Fetal, Transition and Neonatal Circulation: Divya Mishra Dept of PediatricsDocument37 pagesFetal, Transition and Neonatal Circulation: Divya Mishra Dept of PediatricsMathan KarthikNo ratings yet
- Cardio BasicsDocument8 pagesCardio Basicsanandn22No ratings yet
- CHD Fetal CirculationDocument31 pagesCHD Fetal CirculationNandita ChatterjeeNo ratings yet
- (Medbook4u Com) IllBaby1Document693 pages(Medbook4u Com) IllBaby1Certificate SurrenderNo ratings yet
- Cardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPDocument90 pagesCardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPAndra HijratulNo ratings yet
- Congenital Heart Defect EDITDocument57 pagesCongenital Heart Defect EDITnicholasacquah680No ratings yet
- Chapter 020Document54 pagesChapter 020Mar3RDi MusicNo ratings yet
- VHD: Types, Causes, Symptoms & ManagementDocument42 pagesVHD: Types, Causes, Symptoms & ManagementareeparambilNo ratings yet
- Pediatric Echocardiography: Understanding Congenital Heart DefectsDocument159 pagesPediatric Echocardiography: Understanding Congenital Heart DefectsSergiu NiculitaNo ratings yet
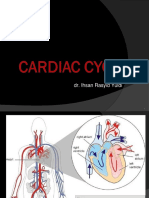
- Dr. Ihsan Rasyid Yuldi's Guide to the Cardiac CycleDocument37 pagesDr. Ihsan Rasyid Yuldi's Guide to the Cardiac CycleEltika utariNo ratings yet
- Circulatory System OverviewDocument65 pagesCirculatory System OverviewgedesuryawanNo ratings yet
- Thorak SDocument71 pagesThorak Srizkynugroho15No ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- MITRAL STENOSIS: CAUSES, SYMPTOMS AND TREATMENTDocument17 pagesMITRAL STENOSIS: CAUSES, SYMPTOMS AND TREATMENTMuhammad Khoirul SodiqNo ratings yet
- Valvular Heart Disease: Etiology PathophysiologyDocument34 pagesValvular Heart Disease: Etiology PathophysiologyensiNo ratings yet
- Step 1 ShartzDocument333 pagesStep 1 ShartzDaniella Vazquez100% (1)
- Cardiac Diseases in ChildrenDocument66 pagesCardiac Diseases in ChildrenHarmas Novryan FarezaNo ratings yet
- Pericardial Disease: Adel Hasanin Ahmed 1Document5 pagesPericardial Disease: Adel Hasanin Ahmed 1Shaz ChindhyNo ratings yet
- Valvular Heart Disease: Mitral Stenosis, Mitral Regurgitation, Aortic StenosisDocument79 pagesValvular Heart Disease: Mitral Stenosis, Mitral Regurgitation, Aortic StenosisDumora FatmaNo ratings yet
- Mitral StenosisDocument17 pagesMitral StenosisMuhammad Alauddin Sarwar100% (8)
- (K7) Valvular Heart DiseaseDocument79 pages(K7) Valvular Heart DiseaseXeniel AlastairNo ratings yet
- Cardiac SurgeryDocument110 pagesCardiac SurgeryChristopher McAndrew100% (1)
- Dynamic Auscultation of Heart Sounds and Murmurs: W. Lane Edwards, JR., MSN, ARNP, ANPDocument43 pagesDynamic Auscultation of Heart Sounds and Murmurs: W. Lane Edwards, JR., MSN, ARNP, ANPDanielleNo ratings yet
- Fisiologi Jantung KananDocument8 pagesFisiologi Jantung KananagungNo ratings yet
- Cardiac ImagingDocument118 pagesCardiac ImagingSay DieukayNo ratings yet
- Pleno Minggu 3 Blok 3.2Document57 pagesPleno Minggu 3 Blok 3.2ima_nekonayagiNo ratings yet
- PE of Common CVSDocument105 pagesPE of Common CVSKaushal RudaniNo ratings yet
- KP 2.3.1.6Document42 pagesKP 2.3.1.6Taufiqurrahman HabibNo ratings yet
- Cardiac Basics Student Copy.Document31 pagesCardiac Basics Student Copy.Preet KaurNo ratings yet
- PA Projection AP ProjectionDocument64 pagesPA Projection AP ProjectionMiaMDNo ratings yet
- Cardiovasucular Problems in Children: Niranjana Shalini. M.SC (N) Assistant ProfessorDocument79 pagesCardiovasucular Problems in Children: Niranjana Shalini. M.SC (N) Assistant ProfessorNIRANJANA SHALININo ratings yet
- The Heart: (See An Anatomy Book and Chapter 9 of G&H)Document30 pagesThe Heart: (See An Anatomy Book and Chapter 9 of G&H)raanja2No ratings yet
- Heart Failure Minus NarrationDocument43 pagesHeart Failure Minus NarrationHamza AldiriNo ratings yet
- CVS Embryology Questions and Study Guide - Quizlet Flashcards by Hugo - OxfordDocument5 pagesCVS Embryology Questions and Study Guide - Quizlet Flashcards by Hugo - OxfordAzizNo ratings yet
- 3 - Valvular Heart DiseasesDocument43 pages3 - Valvular Heart DiseasesHamzehNo ratings yet
- The Cardiovascular System in ActionDocument28 pagesThe Cardiovascular System in ActionCharmen Evangelio Pabilona-FloresNo ratings yet
- Fetal Cardiology: A Practical Approach to Diagnosis and ManagementFrom EverandFetal Cardiology: A Practical Approach to Diagnosis and ManagementNo ratings yet
- ATLS Thermal Injuries PDFDocument9 pagesATLS Thermal Injuries PDFKhayla RayBernadine MancaoRondobioNo ratings yet
- Electrophysiological Properties of Cardiac MyocytesDocument39 pagesElectrophysiological Properties of Cardiac Myocytesapi-19916399No ratings yet
- PNF 7 The Effect of Trunk Stability Excercise Using Stabilising ReservalDocument9 pagesPNF 7 The Effect of Trunk Stability Excercise Using Stabilising ReservalAnonymous j0xAgHs3No ratings yet
- Soal Semester Genapbahasa Inggris Pemintan XiDocument8 pagesSoal Semester Genapbahasa Inggris Pemintan XiJhon ferizalNo ratings yet
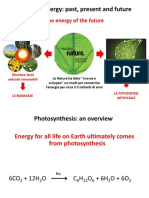
- 5 FotosintesiDocument29 pages5 FotosintesiSerena DamianNo ratings yet
- Autonomic Nervus System: Dr. Meida Sofyana, MbiomedDocument26 pagesAutonomic Nervus System: Dr. Meida Sofyana, MbiomedAyu Tiara FitriNo ratings yet
- Lecture - 5 PDFDocument5 pagesLecture - 5 PDFDavid JokerNo ratings yet
- Blood Group: Made By:-Vedant PatelDocument18 pagesBlood Group: Made By:-Vedant PatelVedant PatelNo ratings yet
- Adrenergic Drugs Classification and UsesDocument2 pagesAdrenergic Drugs Classification and UsesSunshine_Bacla_4275No ratings yet
- Cardiac ArrhythmiasDocument11 pagesCardiac ArrhythmiasChino Paolo SamsonNo ratings yet
- 1.1 The Human Respiratory System - 1.2 Gas Exchange - 1.3 BreathingDocument26 pages1.1 The Human Respiratory System - 1.2 Gas Exchange - 1.3 BreathingAla' ShehadehNo ratings yet
- ASTHMADocument16 pagesASTHMAAyesigwa Gerald96100% (1)
- COLD TEMPERATURE EFFECTDocument4 pagesCOLD TEMPERATURE EFFECTRomydaQurrotinA'yuniNo ratings yet
- Optimize Your Brain S Cleansing Mechanism 2414Document9 pagesOptimize Your Brain S Cleansing Mechanism 2414WilberellisNo ratings yet
- (ACC ENGLISH) ASKEP HiperglikemiaDocument11 pages(ACC ENGLISH) ASKEP HiperglikemiaWenNo ratings yet
- M1 Introduction To Anatomy and PhysiologyDocument4 pagesM1 Introduction To Anatomy and PhysiologyMeteor 858No ratings yet
- Untitled26 PDFDocument14 pagesUntitled26 PDFElizabeth LeonNo ratings yet
- Adult Cardiac Arrest AlgoritmaDocument1 pageAdult Cardiac Arrest AlgoritmaYouniehacibie Ichisky ChildNo ratings yet
- SNB (SN) Question 2015 July 29Document4 pagesSNB (SN) Question 2015 July 29phyo shan100% (2)
- Laporan Kunjungan Karyawn Rich's Jan-Des 2022Document19 pagesLaporan Kunjungan Karyawn Rich's Jan-Des 2022Andri AngbawiNo ratings yet
- Free Anatomy Homework HelpDocument7 pagesFree Anatomy Homework Helpbcdanetif100% (1)
- Highlights2020 Essay eDocument7 pagesHighlights2020 Essay eS3MT-10 Fong Lok ChingNo ratings yet
- Ecg Stemi: Sequence of Changes in Evolving STEMIDocument3 pagesEcg Stemi: Sequence of Changes in Evolving STEMIFajar AgNo ratings yet
- Introduction To Emergency Nursing Concepts FinalDocument128 pagesIntroduction To Emergency Nursing Concepts FinalKarren FernandezNo ratings yet
- Biology worksheet answersDocument2 pagesBiology worksheet answersAziyaNo ratings yet
- Nursing Assessment, Diagnosis, Intervention, and EvaluationDocument5 pagesNursing Assessment, Diagnosis, Intervention, and EvaluationNikael Patun-ogNo ratings yet
- Case Study 5 - DESOASIDODocument2 pagesCase Study 5 - DESOASIDOEDDREI PAULLYNNE DESOASIDONo ratings yet
- ADD 00062218 Hematology Learning GuideDocument52 pagesADD 00062218 Hematology Learning GuideSangel LópezNo ratings yet
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- San Vicente West, Urdaneta CityDocument5 pagesSan Vicente West, Urdaneta CityTIPAY, EMELIE L.No ratings yet