You might also like
- Microbiology of Ocular InfectionsDocument71 pagesMicrobiology of Ocular InfectionsryanradifanNo ratings yet
- MLC Area 08 - Accommodation - WHO - 2011-05-00 - IHR (2005) - Handbook For Inspection of Ships and Issuance of Ship Sanitation CertificatesDocument134 pagesMLC Area 08 - Accommodation - WHO - 2011-05-00 - IHR (2005) - Handbook For Inspection of Ships and Issuance of Ship Sanitation CertificatesMilan ChaddhaNo ratings yet
- Acinetobacter BaumanniiDocument53 pagesAcinetobacter BaumanniiLaboratorium BorromeusNo ratings yet
- HbA1c Test 1Document11 pagesHbA1c Test 1Mohammed R.HusseinNo ratings yet
- Measurements in EpidemiologyDocument24 pagesMeasurements in EpidemiologyAnand gowda75% (4)
- Kawasaki Disease NCPDocument2 pagesKawasaki Disease NCPRay Jhunel Cemine Pascual100% (2)
- University of Santo Tomas - Medical Technology Diagnostic MicrobiologyDocument5 pagesUniversity of Santo Tomas - Medical Technology Diagnostic Microbiologythedarkwing100% (1)
- Pathophysiology Diagram: Breast Cancer: Predisposing Factors: Precipitating FactorsDocument2 pagesPathophysiology Diagram: Breast Cancer: Predisposing Factors: Precipitating FactorsMarinill Soliman100% (1)
- AcinetobacterDocument44 pagesAcinetobacterhypebeast dopeNo ratings yet
- Sexually Transmitted DiseasesDocument54 pagesSexually Transmitted DiseasesMowlidAbdirahman Ali madaaleNo ratings yet
- Necrotizing Pneumonia and Lung AbscessDocument11 pagesNecrotizing Pneumonia and Lung AbscessIman KhanNo ratings yet
- 10.2 Family Neisseriaceae PDFDocument6 pages10.2 Family Neisseriaceae PDFAnne MorenoNo ratings yet
- Microbio Lec 4 - Microbial Flora in Health and DiseaseDocument2 pagesMicrobio Lec 4 - Microbial Flora in Health and Diseaseapi-374321750% (2)
- Overview of Gram - Negative Rods Enterobacteriaceae & Other Than EnterobacteriaceaeDocument51 pagesOverview of Gram - Negative Rods Enterobacteriaceae & Other Than EnterobacteriaceaeAudhrey BNo ratings yet
- Peptococcus PeptostreptococcusDocument25 pagesPeptococcus PeptostreptococcusIon PopescuNo ratings yet
- Diagnostic Microbiology - : University of Santo Tomas - Medical TechnologyDocument6 pagesDiagnostic Microbiology - : University of Santo Tomas - Medical TechnologyWynlor AbarcaNo ratings yet
- Basic MicrobiologyDocument53 pagesBasic MicrobiologyJohn NirmalNo ratings yet
- Lesson 36Document13 pagesLesson 36Abdelraouf ElmanamaNo ratings yet
- Microb KARDIO 2019Document48 pagesMicrob KARDIO 2019sintia djafarNo ratings yet
- A 2.1.bakteria Gram NegatifDocument39 pagesA 2.1.bakteria Gram NegatifQhus YairyNo ratings yet
- Hospital InfectionsDocument35 pagesHospital InfectionsAna KarlaNo ratings yet
- Acinetobacter, Strenotrophomonas, and Similar Organisms: General DescriptionDocument2 pagesAcinetobacter, Strenotrophomonas, and Similar Organisms: General DescriptionTrisha Dela CruzNo ratings yet
- Gram-Positive BacteriaDocument54 pagesGram-Positive BacteriaNurul AnisshaNo ratings yet
- INFEKSI CompressedDocument2 pagesINFEKSI CompressedAsha TumanggorNo ratings yet
- Acute Gastroenteritis in Children Acute Gastroenteritis in ChildrenDocument28 pagesAcute Gastroenteritis in Children Acute Gastroenteritis in ChildrenFernando AnibanNo ratings yet
- Non-Sporing Anaerobes: ASHWINI S. DESHPANDE (Department of Microbiology)Document30 pagesNon-Sporing Anaerobes: ASHWINI S. DESHPANDE (Department of Microbiology)Loukik TaysheteNo ratings yet
- Lec4 TransDocument23 pagesLec4 TransErika PatarayNo ratings yet
- Groupone MycologyDocument14 pagesGroupone MycologyTilahun TesemaNo ratings yet
- Cwpams Joint TrainingDocument318 pagesCwpams Joint TrainingHarriet TembaNo ratings yet
- Apurba 1Document16 pagesApurba 1ayushya.mbbsNo ratings yet
- 7.01-Medically Important Bacteria II (Part I)Document54 pages7.01-Medically Important Bacteria II (Part I)danNo ratings yet
- Pathologic and NonDocument11 pagesPathologic and NonAisha DoreenNo ratings yet
- Medical Bacteriology, Henrys Laboratory MedicineDocument43 pagesMedical Bacteriology, Henrys Laboratory MedicineRikkachuNo ratings yet
- Lec8 Infectious DiseasesDocument32 pagesLec8 Infectious DiseasesmanuelNo ratings yet
- Example and List of Medically Significant BacteriaDocument6 pagesExample and List of Medically Significant BacteriaJhe TesoroNo ratings yet
- Chapter 5 Medically Most Important BacteriaDocument5 pagesChapter 5 Medically Most Important BacteriaclarisseNo ratings yet
- Enterobacter With Mucoid Colonies) : Clinical BacteriologyDocument29 pagesEnterobacter With Mucoid Colonies) : Clinical BacteriologyIra ElizagaNo ratings yet
- Basic Microbiology For 2014 Ver1Document27 pagesBasic Microbiology For 2014 Ver1Dr. Mussa QamerNo ratings yet
- Summary Final 2022Document12 pagesSummary Final 2022Rana zaatrehNo ratings yet
- Penggunaan AB Pada HAIs Aceh 2015Document51 pagesPenggunaan AB Pada HAIs Aceh 2015Dewi PrasetiaNo ratings yet
- Bacteria Classification and DiseaseDocument33 pagesBacteria Classification and DiseaseSyed ShahNo ratings yet
- Kuliah Mikrobiologi Part 1Document34 pagesKuliah Mikrobiologi Part 1Amalia YasminNo ratings yet
- 2013 Article 6Document6 pages2013 Article 6ary wisma dewiNo ratings yet
- ENTEROBACTERIACEAEDocument34 pagesENTEROBACTERIACEAEdrtsotlhe mogolegwaNo ratings yet
- Medically Important Bacteria BookDocument150 pagesMedically Important Bacteria Bookعلي الكوافيNo ratings yet
- 11 - Anaerobic BacteriaDocument68 pages11 - Anaerobic BacteriaJohanna Kate DiestroNo ratings yet
- 1 - 4 Antimicrobial TherapyDocument212 pages1 - 4 Antimicrobial Therapyaleen qawareetNo ratings yet
- DR. KELI MEM203 BacteriologyDocument160 pagesDR. KELI MEM203 Bacteriologykaregagladys90No ratings yet
- Problem 3.01 Nervous System Study Guide 4Document3 pagesProblem 3.01 Nervous System Study Guide 4Monish NaiduNo ratings yet
- Bacterial Meningitis CaseDocument24 pagesBacterial Meningitis CaseALI MUMTAZNo ratings yet
- Opportunistic MycosesDocument28 pagesOpportunistic MycosesSally ElhadadNo ratings yet
- Lab Sheet - Capsule StainingDocument2 pagesLab Sheet - Capsule Stainingbliss polleyNo ratings yet
- Anaerobic Infection, by MahrukhDocument11 pagesAnaerobic Infection, by MahrukhImran Niaz KhanNo ratings yet
- Chapter 8 - Infectious DiseasesDocument17 pagesChapter 8 - Infectious DiseasesAgnieszka WisniewskaNo ratings yet
- 2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Document52 pages2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Tonny YuliantoNo ratings yet
- Chapter 7 Normal Human MicrobiotaDocument34 pagesChapter 7 Normal Human MicrobiotaAkbar SaleemNo ratings yet
- Summary of The Lecture On Lesson 21Document8 pagesSummary of The Lecture On Lesson 21hari dharshanNo ratings yet
- Gram Negative HandoutDocument1 pageGram Negative HandoutAnna CrisNo ratings yet
- Fungal Causing DiseasesDocument9 pagesFungal Causing DiseasesSAMSON, MAXZENE ANICKANo ratings yet
- Dr. Abdelhakam Aldigeal Enterobacter CitrobacterDocument22 pagesDr. Abdelhakam Aldigeal Enterobacter CitrobacterAbdelhakam AliNo ratings yet
- General Pathology of Infectious DiseasesDocument42 pagesGeneral Pathology of Infectious Diseasesapi-19916399No ratings yet
- Articulo E.coliDocument19 pagesArticulo E.coliHelio GrullónNo ratings yet
- Anaerobic Bacteria - Infectious Disease and Antimicrobial AgentsDocument10 pagesAnaerobic Bacteria - Infectious Disease and Antimicrobial AgentsAhsan KhanNo ratings yet
- Mikroba Terkait HaisDocument64 pagesMikroba Terkait HaisDwi JayantiNo ratings yet
- of PHDDocument129 pagesof PHDHimanshu GargNo ratings yet
- High Risk Pregnancy 1Document26 pagesHigh Risk Pregnancy 1alinaziyad3No ratings yet
- Preventive OphthalmologyDocument2 pagesPreventive Ophthalmologysarguss14100% (1)
- Daily UrduDocument4 pagesDaily UrduFurqanAftabNo ratings yet
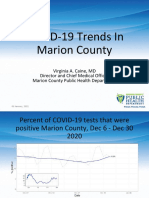
- Marion County Public Health Update 01.07.21Document15 pagesMarion County Public Health Update 01.07.21Last DayNo ratings yet
- (Hodder Arnold Publication) Paul Goldsmith, Robert Semple-Case Histories For The MRCP - A Hodder Arnold Publication (2004)Document328 pages(Hodder Arnold Publication) Paul Goldsmith, Robert Semple-Case Histories For The MRCP - A Hodder Arnold Publication (2004)Ahmad ElgazzarNo ratings yet
- Vasculitis SyndromesDocument1 pageVasculitis SyndromesamanNo ratings yet
- CASE 1 GBS ADULT PHARMACISTs CARE PLANDocument3 pagesCASE 1 GBS ADULT PHARMACISTs CARE PLANquina mjNo ratings yet
- Bloodborne Pathogens PPT v-03!01!17Document44 pagesBloodborne Pathogens PPT v-03!01!17kunalphalswal0005No ratings yet
- Systemic MycosisDocument15 pagesSystemic Mycosisapi-19969058No ratings yet
- Quotes On VaccinesDocument6 pagesQuotes On VaccinesKris BargerNo ratings yet
- Aids HivDocument140 pagesAids HivKarina Flores RezpkaNo ratings yet
- Vital Statistics FormulaDocument3 pagesVital Statistics Formulaluhhh celllNo ratings yet
- Therapy LV CNS 4th Year KirubelDocument156 pagesTherapy LV CNS 4th Year Kirubelpblinder1319No ratings yet
- TOP 10 MORBIDITY CASES of CIRCULATORY DISEASES in CALBARZON - 2015-2022-SignedDocument3 pagesTOP 10 MORBIDITY CASES of CIRCULATORY DISEASES in CALBARZON - 2015-2022-SignedKaguraNo ratings yet
- Primary ComplexDocument12 pagesPrimary ComplexLevi PosadasNo ratings yet
- PSMID COVID TX Guidelines V.3.31.20a PDFDocument62 pagesPSMID COVID TX Guidelines V.3.31.20a PDFRenz Marion AlemaniaNo ratings yet
- Clinical Treatment of Rabbits Experimentally Infected With Staphylococcus Aureus Using Different AntibioticsDocument4 pagesClinical Treatment of Rabbits Experimentally Infected With Staphylococcus Aureus Using Different Antibioticsarum pratiwiNo ratings yet
- What Are Foodborne IllnessesDocument2 pagesWhat Are Foodborne IllnessesDavid Lara RodriguezNo ratings yet
- Ade Egie Prayogi - Perbaikan InggrisDocument6 pagesAde Egie Prayogi - Perbaikan InggrisAde Egie PrayogiNo ratings yet
- Intramuscular Injection in Patients With Bleeding Disorders Guidance For Patients and CliniciansDocument6 pagesIntramuscular Injection in Patients With Bleeding Disorders Guidance For Patients and CliniciansRawan KHNo ratings yet
- Baby Massage Consultation Form - November 2017Document1 pageBaby Massage Consultation Form - November 2017api-257327106No ratings yet
- Artrite REATIVAsexualmente ADQUIRIDADocument10 pagesArtrite REATIVAsexualmente ADQUIRIDAYgor AlbuquerqueNo ratings yet
- CNS TumorDocument32 pagesCNS TumorBbem ooNo ratings yet