You might also like
- Maitland Joint MobilizationDocument40 pagesMaitland Joint Mobilizationkitu_alagappan472060% (5)
- Hip ExaminationDocument84 pagesHip ExaminationDeepak KumarNo ratings yet
- Hernia and Acute Abdomen MCQDocument44 pagesHernia and Acute Abdomen MCQShriyansh Chahar50% (4)
- MODULE 2 Ichthyology - SECTION 5 Shark Anatomy and Dogfish Dissection PDFDocument27 pagesMODULE 2 Ichthyology - SECTION 5 Shark Anatomy and Dogfish Dissection PDFElishae SamonteNo ratings yet
- Lower Crossed SyndromeDocument8 pagesLower Crossed SyndromeThaseen75% (4)
- Inservice For LoyolaDocument13 pagesInservice For Loyolaapi-659939847No ratings yet
- 1-5-22 OMM Repro Considerations MasterDocument67 pages1-5-22 OMM Repro Considerations MasterTanner HancockNo ratings yet
- Hip Syndromes - Shirley SahrmanDocument17 pagesHip Syndromes - Shirley SahrmanSonia LvNo ratings yet
- Sacroiliac Joint Pain: Heidi Prather, DO and Devyani Hunt, MDDocument14 pagesSacroiliac Joint Pain: Heidi Prather, DO and Devyani Hunt, MDNurfitrianti ArfahNo ratings yet
- Ilio-Sacral Diagnosis and Treatment, Part One-Shears, Upslips and DownslipsDocument4 pagesIlio-Sacral Diagnosis and Treatment, Part One-Shears, Upslips and Downslipstachy2006No ratings yet
- Sacroiliac Joint Dysfunction: Causes, Symptoms and TreatmentDocument58 pagesSacroiliac Joint Dysfunction: Causes, Symptoms and TreatmentBelle Sakunrat SarikitNo ratings yet
- Chap 14-1Document29 pagesChap 14-1abdul hannanNo ratings yet
- Sacroiliac 201: Dysfunction and Management: A Biomechanical SolutionDocument9 pagesSacroiliac 201: Dysfunction and Management: A Biomechanical Solutionปฏิเวธคงไพจิตรวงศ์No ratings yet
- Sacroiliac jointDocument72 pagesSacroiliac jointmariajaved0089No ratings yet
- Classic vs. Functional Movement in PT: Restoring Spine and Hip MobilityDocument37 pagesClassic vs. Functional Movement in PT: Restoring Spine and Hip MobilityDevi SiswaniNo ratings yet
- 399 753 1 SMDocument8 pages399 753 1 SMmuhammad untungNo ratings yet
- A Comprehensive Treatment Guide For Low Back Strains and SprainsDocument17 pagesA Comprehensive Treatment Guide For Low Back Strains and SprainsHoan TrầnNo ratings yet
- Low Back Pain: Rezki Amalia NurshalDocument74 pagesLow Back Pain: Rezki Amalia NurshalRezki Amalia NurshalNo ratings yet
- Ankylosing SpondylitisDocument31 pagesAnkylosing SpondylitisArathy100% (1)
- SIJ Presentation Slides PDFDocument41 pagesSIJ Presentation Slides PDFPhillip VoglisNo ratings yet
- Sacroiliac Joint PainDocument10 pagesSacroiliac Joint PainLev Kalika100% (2)
- Approach To A Patient With Low Back Ache: DR - Ankur BatraDocument104 pagesApproach To A Patient With Low Back Ache: DR - Ankur BatraAnkur Batra100% (1)
- Sacroiliac Joint Dysfunction: Pathophysiology, Diagnosis, and TreatmentDocument8 pagesSacroiliac Joint Dysfunction: Pathophysiology, Diagnosis, and TreatmentNurfitrianti ArfahNo ratings yet
- Anks PondDocument32 pagesAnks Pondmiskiah lainunNo ratings yet
- Sacro Occipital Techniques Category Two A Remedy For Fixated Thinking 1352662451Document7 pagesSacro Occipital Techniques Category Two A Remedy For Fixated Thinking 1352662451rcastello20No ratings yet
- Low Back Ache: Capt PramodDocument67 pagesLow Back Ache: Capt PramodPramod MahenderNo ratings yet
- Lumber SpondylosisDocument25 pagesLumber SpondylosisYusrah SaniNo ratings yet
- TECH 524 - Palpation II (Castellucci) 9 2015Document12 pagesTECH 524 - Palpation II (Castellucci) 9 2015Robert StraubNo ratings yet
- SpondylolysisDocument13 pagesSpondylolysisYang100% (1)
- WMSD Dentist 2566Document77 pagesWMSD Dentist 2566pachara.p65No ratings yet
- Hip PT AssessmentDocument57 pagesHip PT Assessmentkrissh20No ratings yet
- Assessmentofshoulder 180107041721Document36 pagesAssessmentofshoulder 180107041721Chandra PrabhaNo ratings yet
- Sacroiliac Joint DysfunctionDocument2 pagesSacroiliac Joint DysfunctionMinnymin OnumaNo ratings yet
- Review of Literature: Presenting By: Monika S. Kulkarni 1 Year MPT Department of Orthopaedic Manual TherapyDocument44 pagesReview of Literature: Presenting By: Monika S. Kulkarni 1 Year MPT Department of Orthopaedic Manual TherapyANKITA SHETTYNo ratings yet
- The Painful Shoulder - Part I. Clinical Evaluation PDFDocument17 pagesThe Painful Shoulder - Part I. Clinical Evaluation PDFOscar FrizziNo ratings yet
- Evidence of Altered Lumbopelvic Muscle Recruitment in The Presence of SI Joint Pain.Document8 pagesEvidence of Altered Lumbopelvic Muscle Recruitment in The Presence of SI Joint Pain.Christian Donoso AguilarNo ratings yet
- Lumbopelvic Stability: SyllabusDocument13 pagesLumbopelvic Stability: Syllabusrapannika100% (3)
- Hip Application SolutionsDocument3 pagesHip Application SolutionsDNo ratings yet
- SI Joint Dysfunction Treatment Protocols: Presenter NotesDocument15 pagesSI Joint Dysfunction Treatment Protocols: Presenter NotesMichel BakkerNo ratings yet
- Varieties of Spondylolisthesis: (A) Normal, (B) Congenital, (C) Isthmic, (D) Traumatic, (E) Degenerative, and (F) PathologicalDocument5 pagesVarieties of Spondylolisthesis: (A) Normal, (B) Congenital, (C) Isthmic, (D) Traumatic, (E) Degenerative, and (F) PathologicalYashaswi ANo ratings yet
- Psoas Insufficiency and Its Role in Sacroiliac DysfunctionDocument45 pagesPsoas Insufficiency and Its Role in Sacroiliac DysfunctionAlexandru Nechifor100% (1)
- Lumbo-Pelvic Stability and Back Pain: What's The Link?Document8 pagesLumbo-Pelvic Stability and Back Pain: What's The Link?atul-heroNo ratings yet
- Assessment of the Musculoskeletal SystemDocument35 pagesAssessment of the Musculoskeletal SystemChristine Joy MolinaNo ratings yet
- Orthopedic Diseases: Low Back Pain (LBP)Document12 pagesOrthopedic Diseases: Low Back Pain (LBP)Libra Boy KokoNo ratings yet
- Doug Keller - Pelvic Balance Slides - Part TwoDocument41 pagesDoug Keller - Pelvic Balance Slides - Part Twoshivnair100% (8)
- Sherin Seminar 1 Combined Movements AssessmentDocument47 pagesSherin Seminar 1 Combined Movements AssessmentANKITA SHETTYNo ratings yet
- The Painful Shoulder - Part I. Clinical Evaluation - American Family PhysicianDocument9 pagesThe Painful Shoulder - Part I. Clinical Evaluation - American Family PhysicianAngelaNo ratings yet
- Lecture Scap Malaga 2Document47 pagesLecture Scap Malaga 2danielaNo ratings yet
- The Effect of Thoracic Spine MobilizationDocument4 pagesThe Effect of Thoracic Spine MobilizationEric SimasNo ratings yet
- Musculoskeletal System Student HandoutDocument35 pagesMusculoskeletal System Student HandoutSheNo ratings yet
- Low Back Pain: Anwar SuhaimiDocument24 pagesLow Back Pain: Anwar SuhaimiAfonso RochaNo ratings yet
- Lec2 The Spine 2Document37 pagesLec2 The Spine 2sana mumtazNo ratings yet
- Spinal Biomechanics: Posture AnalysisDocument74 pagesSpinal Biomechanics: Posture AnalysisDoddy RenaLdoNo ratings yet
- Naskah PublikasiDocument15 pagesNaskah PublikasiSuci AisyahNo ratings yet
- The McKenzieDocument57 pagesThe McKenzieStefan VladNo ratings yet
- Posture Dr. Dr. MY, SP KFR-KDocument67 pagesPosture Dr. Dr. MY, SP KFR-KCikupaNo ratings yet
- Si JointDocument6 pagesSi JointSyifa RahmadantiNo ratings yet
- Shoulder Assessment: Ayesha RazzaqDocument47 pagesShoulder Assessment: Ayesha RazzaqayeshaNo ratings yet
- Core Muscle Strengthening in The AthleteDocument48 pagesCore Muscle Strengthening in The AthleteNicu Tanase-RaduNo ratings yet
- PostureDocument85 pagesPostureDr.Debanjan Mondal (pt)100% (1)
- 1 Askep Low Back PainDocument16 pages1 Askep Low Back PainBr Komarudin100% (1)
- Indictment Against Anders Behring Breivik - 07032012Document18 pagesIndictment Against Anders Behring Breivik - 07032012Fredrik WalløeNo ratings yet
- Laparoscopic Repair of Inguinal HerniaDocument12 pagesLaparoscopic Repair of Inguinal Herniawadhe omara100% (1)
- 5b9f87df82236UG Syllabus (MBBS) AIIMS RaipurDocument8 pages5b9f87df82236UG Syllabus (MBBS) AIIMS RaipurBri MinNo ratings yet
- Lecture - One: Anatomy of The Anterior Abdominal WallDocument25 pagesLecture - One: Anatomy of The Anterior Abdominal WallAhmed OudahNo ratings yet
- Anatomy OSPE AnswersDocument3 pagesAnatomy OSPE AnswersIdham Ahmad NazliNo ratings yet
- Anatomy and Function of the LungsDocument4 pagesAnatomy and Function of the Lungs31 PASION, ROCHELLE C.No ratings yet
- CVS/ The Blood Vessels: by DR - Ahmed Avdel MandaniDocument27 pagesCVS/ The Blood Vessels: by DR - Ahmed Avdel MandaniSerwan J AbdulrahmanNo ratings yet
- 1.the AbdomenDocument21 pages1.the AbdomenLeona Tinotenda ManjeruNo ratings yet
- Answers Biruni Uni, Faculty of Dentistry Phase 2 Midterm Exam 2021Document8 pagesAnswers Biruni Uni, Faculty of Dentistry Phase 2 Midterm Exam 2021ArinaNo ratings yet
- Abdominal ExaminationDocument54 pagesAbdominal ExaminationGemmalene Pacleb100% (4)
- Anatomy CoronaryDocument6 pagesAnatomy Coronarybri bugelNo ratings yet
- HBS-Distance Learning - Heart Diagram LabelingDocument4 pagesHBS-Distance Learning - Heart Diagram LabelingCin CinNo ratings yet
- Lumbar Spine Follower LoadDocument5 pagesLumbar Spine Follower LoadShiva0% (1)
- LAB EXERCISE 1 Organization of The Human Body - BS PSYCH 1 B 1Document10 pagesLAB EXERCISE 1 Organization of The Human Body - BS PSYCH 1 B 1Louise BarrientosNo ratings yet
- Anatomy For The Gynecologic OncologistDocument70 pagesAnatomy For The Gynecologic OncologistjroshsperlingNo ratings yet
- Jurnal Imejing DiagnostikDocument5 pagesJurnal Imejing DiagnostikMita HmNo ratings yet
- Abdomen - 1Document48 pagesAbdomen - 1rohanshah1No ratings yet
- Precise Neurovascular Anatomy For Radical Hysterectomy: Shingo Fujii Kentaro SekiyamaDocument217 pagesPrecise Neurovascular Anatomy For Radical Hysterectomy: Shingo Fujii Kentaro SekiyamaIrina100% (3)
- 01 CT Anatomia HigadoDocument14 pages01 CT Anatomia HigadoPablo TalamantesNo ratings yet
- Strapping Applications For Hypotonia, Posture, and Trunk AlignmentDocument6 pagesStrapping Applications For Hypotonia, Posture, and Trunk AlignmentMaria De Los AngelesNo ratings yet
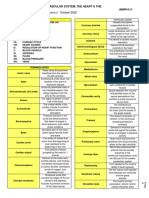
- 1.08 - The Cardiovascular System, The Heart & The Blood VesselsDocument9 pages1.08 - The Cardiovascular System, The Heart & The Blood Vessels13PLAN, SENTH RUEN, ANo ratings yet
- Icd XDocument30 pagesIcd Xrsud butengNo ratings yet
- Groin ProtocolDocument7 pagesGroin ProtocolElloide PajutanNo ratings yet
- DDLT RetrievalDocument33 pagesDDLT RetrievalPriya RanjanNo ratings yet
- ManualDocument95 pagesManualcristina_c_43No ratings yet
- Carcinoma StomachDocument43 pagesCarcinoma StomachRukman Mecca100% (1)
- Stomach: Presented By: Dushyanth MDocument17 pagesStomach: Presented By: Dushyanth MSanjay NaikNo ratings yet
- Coccyx PDFDocument5 pagesCoccyx PDFtechzonesNo ratings yet