You might also like
- Lichen Planus, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandLichen Planus, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- What Are The Dangers of Sodium Silicate?: InhalationDocument10 pagesWhat Are The Dangers of Sodium Silicate?: InhalationAlaa SalemNo ratings yet
- Partial-Thickness (Second-Degree) Involves The Epidermis and Varying Degrees of TheDocument7 pagesPartial-Thickness (Second-Degree) Involves The Epidermis and Varying Degrees of Thegreat_loverboy09No ratings yet
- PEDIA Ear and ThroatDocument174 pagesPEDIA Ear and ThroatmatrixtrinityNo ratings yet
- Hydrocarbon Poisoning EditDocument20 pagesHydrocarbon Poisoning Editrafa niwasNo ratings yet
- GI Disorders Part 1Document17 pagesGI Disorders Part 1LillabinNo ratings yet
- GIT - Dr. Allam 2021 PDFDocument47 pagesGIT - Dr. Allam 2021 PDFMohammedNo ratings yet
- AlkalisDocument14 pagesAlkalisSamona khanNo ratings yet
- Integumentary System Review - BurnsDocument52 pagesIntegumentary System Review - BurnsmikErlhNo ratings yet
- Report On Ethiology, Epidemiology, Pathogenesis, Clinical Features and The Treatment Principles of Cholera. Dehydration - Rehydration.Document2 pagesReport On Ethiology, Epidemiology, Pathogenesis, Clinical Features and The Treatment Principles of Cholera. Dehydration - Rehydration.Adnan Akram, MD (Latvia)No ratings yet
- RP RPDocument6 pagesRP RPEliezah RodriguezNo ratings yet
- Caustic InjuryDocument26 pagesCaustic InjuryGino FTNo ratings yet
- Pathology-GIT Answered EssayDocument33 pagesPathology-GIT Answered EssayRancesh FamoNo ratings yet
- Corrosive Lesions of OesophagusDocument17 pagesCorrosive Lesions of OesophagusAdi VirnawanNo ratings yet
- Kerosene Toxicity - 1657101641Document22 pagesKerosene Toxicity - 1657101641Mohil PratapNo ratings yet
- CHEMICAL TERRORISM AGENTS AND SYNDROMES: Watch For These Signs and SymptomsDocument2 pagesCHEMICAL TERRORISM AGENTS AND SYNDROMES: Watch For These Signs and Symptomsfrankzy_coolNo ratings yet
- Corrosive Injury 20061227-1Document23 pagesCorrosive Injury 20061227-1ostaz2000No ratings yet
- Bleach PresentationDocument22 pagesBleach PresentationMohil PratapNo ratings yet
- Alcohols Ethanol, MethanolDocument55 pagesAlcohols Ethanol, MethanoljayNo ratings yet
- Blood AgentsDocument6 pagesBlood AgentsAngelica Orbase BelmonteNo ratings yet
- Gastrointestinal SystemDocument8 pagesGastrointestinal Systemtheglobalnursing100% (1)
- Oral RevalidaDocument3 pagesOral RevalidaJaye DangoNo ratings yet
- High Risk PreschoolerDocument7 pagesHigh Risk PreschoolerAngela Del CastilloNo ratings yet
- General Medicine Practical NotesDocument33 pagesGeneral Medicine Practical Notessaakshi parshionikarNo ratings yet
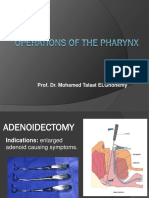
- 3-Pharynx. Operation of The PharynxDocument13 pages3-Pharynx. Operation of The PharynxislamNo ratings yet
- Esophageal Disorders: Suazo, Trisha Mae S. 3BSN-ADocument11 pagesEsophageal Disorders: Suazo, Trisha Mae S. 3BSN-AKenneth OpinaNo ratings yet
- 24 Anorectal ConditionsDocument55 pages24 Anorectal ConditionsRaisa CleizeraNo ratings yet
- Riaz Gul AHN Unit 1Document106 pagesRiaz Gul AHN Unit 1Riaz Gul RindNo ratings yet
- Obstruction EDocument10 pagesObstruction ECorina MunteanuNo ratings yet
- Deputy Provost MCHDocument250 pagesDeputy Provost MCHrahmatullahqueenmercyNo ratings yet
- What Is A Toxin ?: Toxicology Is The Study of How Natural or ManDocument48 pagesWhat Is A Toxin ?: Toxicology Is The Study of How Natural or ManMds UniNo ratings yet
- Week 13 NCMB 312 Lect NotesDocument18 pagesWeek 13 NCMB 312 Lect NotesAngie BaylonNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- Biowarfare AgentsDocument71 pagesBiowarfare AgentsIan GabritoNo ratings yet
- Cystic FibrosisDocument45 pagesCystic FibrosisAbong Che InnocentNo ratings yet
- Common Health Problems in PreschoolersDocument22 pagesCommon Health Problems in PreschoolersClaire Alvarez OngchuaNo ratings yet
- 03 AmoebiasisDocument42 pages03 AmoebiasisKing IvyNo ratings yet
- AmoebiasisDocument64 pagesAmoebiasisLarry MathisNo ratings yet
- LectureokokDocument31 pagesLectureokokDewivvNo ratings yet
- Group SixDocument16 pagesGroup SixselormniiqNo ratings yet
- PWM Olly Indrajani 2015Document45 pagesPWM Olly Indrajani 2015Dwi WulandariNo ratings yet
- ABC Lecture NotesDocument7 pagesABC Lecture NotesLady Shayne YapNo ratings yet
- GERDDocument12 pagesGERDايمن منصرNo ratings yet
- Communicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistDocument846 pagesCommunicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistGrn Mynjrkxz100% (1)
- Toxic Gases & Their EffectsDocument28 pagesToxic Gases & Their Effectsavula43No ratings yet
- Urticaria بورDocument19 pagesUrticaria بورعبدالرحمن طارق عبدالله صالحNo ratings yet
- Life-Cycle of Entamoeba HistolyticaDocument30 pagesLife-Cycle of Entamoeba Histolyticasonata38No ratings yet
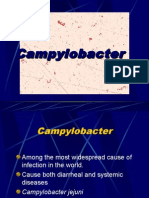
- Salmonella, Campylobacter, Yersinia Enterocolitica and Shigella InfectionsDocument3 pagesSalmonella, Campylobacter, Yersinia Enterocolitica and Shigella InfectionsKelvin BolusanNo ratings yet
- PeritonitisDocument14 pagesPeritonitisAyad IdresNo ratings yet
- The System: RespiDocument247 pagesThe System: RespiKatrina PonceNo ratings yet
- NCP GeDocument14 pagesNCP GeSuluhTriUtomoNo ratings yet
- Acute Laryngitis: Li SGD 21 LBM 5Document40 pagesAcute Laryngitis: Li SGD 21 LBM 511juni09No ratings yet
- 17 FfsfafDocument78 pages17 FfsfafAndres Zambrano ArteagaNo ratings yet
- COPD Case PresentationDocument44 pagesCOPD Case PresentationNaresh JeengarNo ratings yet
- Disorder of Rectum and AnusDocument13 pagesDisorder of Rectum and AnusDIANE CLAUDINA GOSOCONo ratings yet
- Sem 14 - Manj y Enf FS - Mamif - Teo - 2022-1Document45 pagesSem 14 - Manj y Enf FS - Mamif - Teo - 2022-1LucilaAnacletoPérezNo ratings yet
- Tropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaDocument95 pagesTropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaadystiNo ratings yet
- 2 A) Hook Worm InfestationDocument24 pages2 A) Hook Worm InfestationMuhammed sherbinNo ratings yet
- Pediatrics Module 3Document2 pagesPediatrics Module 3Cyrus ZalameaNo ratings yet
- Biology Target PaperDocument2 pagesBiology Target PaperAlhan MhmmadNo ratings yet
- 1-Abbreviations of Medical TermsDocument6 pages1-Abbreviations of Medical Termsyuki_teefNo ratings yet
- Genitourinary MCQDocument27 pagesGenitourinary MCQfrabzi67% (3)
- 11.1 Nephron and Urine FormationDocument27 pages11.1 Nephron and Urine FormationAlfi Oktafani100% (1)
- Doctor of Veterinary Medicine: Scheme of Study of Five Years Composit Degree ProgrammeDocument62 pagesDoctor of Veterinary Medicine: Scheme of Study of Five Years Composit Degree ProgrammeAhmed Hassan SamatarNo ratings yet
- Hsslive Xii Zoology Lab Notes by Navas 2024Document100 pagesHsslive Xii Zoology Lab Notes by Navas 2024spookyvibee666No ratings yet
- Determination of Blood GlucoseDocument3 pagesDetermination of Blood GlucoseAki OtaniNo ratings yet
- RNL - 2020 - Haramati - PSW Assessment of Tubular HandoutDocument3 pagesRNL - 2020 - Haramati - PSW Assessment of Tubular HandoutSal PaNo ratings yet
- Peripheral Edema: ReviewDocument7 pagesPeripheral Edema: ReviewVmsdNo ratings yet
- Mantak Chia - Five Elements Nutrition Alphabetic Food ListDocument74 pagesMantak Chia - Five Elements Nutrition Alphabetic Food ListLautaro Risso100% (1)
- Art 3A10.1007 2Fs00259 013 2535 3 PDFDocument477 pagesArt 3A10.1007 2Fs00259 013 2535 3 PDFHerryAsu-songkoNo ratings yet
- Chapter 11 PetroperitoneumDocument32 pagesChapter 11 PetroperitoneumMACON824No ratings yet
- SMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Document16 pagesSMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Azie HarunNo ratings yet
- The Excretory System: Back To TopDocument10 pagesThe Excretory System: Back To TopDANIA PURNAMANo ratings yet
- Acute Renal Failure, Gastrointestinal Bleeding, and Cardiac ArrhythmiaDocument1 pageAcute Renal Failure, Gastrointestinal Bleeding, and Cardiac ArrhythmiaAnonymous 5AgCCdEPcYNo ratings yet
- MCI SyllabusDocument6 pagesMCI SyllabusloocasjNo ratings yet
- Lecture 4 (1of3) - Nephritic SyndromeDocument45 pagesLecture 4 (1of3) - Nephritic SyndromeAliye BaramNo ratings yet
- Renal Tumors in ChickensDocument5 pagesRenal Tumors in ChickensShah NawazNo ratings yet
- Name: Alcazar, Nica Allen: Across DownDocument1 pageName: Alcazar, Nica Allen: Across DownAllenNo ratings yet
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNo ratings yet
- Complete Guide To Urine TheraphyDocument9 pagesComplete Guide To Urine TheraphyNancy Miro100% (4)
- Acute-Renal-Failure Lecture OnlyDocument17 pagesAcute-Renal-Failure Lecture OnlyeyesontheskyNo ratings yet
- Biology - Excretion LabDocument6 pagesBiology - Excretion LabJadie BabyyyNo ratings yet
- Review Final Exam HBSDocument12 pagesReview Final Exam HBSNaomi Hammonds [STUDENT]No ratings yet
- Embryology of Urinary SystemDocument34 pagesEmbryology of Urinary SystemFatimaNo ratings yet
- HLTAAP001 - Horia RevisedDocument74 pagesHLTAAP001 - Horia RevisedYouYou Tube80% (5)
- Renal Calculi Concept Map PathophysiologyDocument3 pagesRenal Calculi Concept Map PathophysiologySharon TanveerNo ratings yet
- DNB Previous QuestionsDocument75 pagesDNB Previous QuestionsShashank PrakashNo ratings yet
- Homeostasis, The Milieu Intérieur, and The Wisdom of The Nephron 2014 PDFDocument10 pagesHomeostasis, The Milieu Intérieur, and The Wisdom of The Nephron 2014 PDFMg GfNo ratings yet
- Clinical MicrosDocument11 pagesClinical MicrosDayledaniel SorvetoNo ratings yet