You might also like
- Hematopoiesis and Anemias GuideDocument85 pagesHematopoiesis and Anemias GuideammarNo ratings yet
- Anemias (1) by DR - Hydi 3rd MBBS-2016Document63 pagesAnemias (1) by DR - Hydi 3rd MBBS-2016Suban GouseNo ratings yet
- Blood Film Staining Effects Educational Document PDFDocument5 pagesBlood Film Staining Effects Educational Document PDFCrisiant DolinaNo ratings yet
- Screening Hbpathies 2012Document15 pagesScreening Hbpathies 2012Fiky setiawanNo ratings yet
- Staphylococcus Aureus - Pseudomonas Putida - Klebsiella OxytocaDocument4 pagesStaphylococcus Aureus - Pseudomonas Putida - Klebsiella OxytocaJeanette RiosNo ratings yet
- Selective MediaDocument10 pagesSelective Mediaprincess_likemist4No ratings yet
- State The Rules or Precautions To Be Observed For Collection of Such SpecimenDocument4 pagesState The Rules or Precautions To Be Observed For Collection of Such SpecimenMarianneTee-ruhNo ratings yet
- Lab Investigation of AnaemiasDocument109 pagesLab Investigation of AnaemiasMadhura ShekatkarNo ratings yet
- Pre-Analytical Considerations in PhlebotomyDocument56 pagesPre-Analytical Considerations in PhlebotomyAngel joyce ValenciaNo ratings yet
- Urinalysis Cases (Revised)Document3 pagesUrinalysis Cases (Revised)Gold NajmNo ratings yet
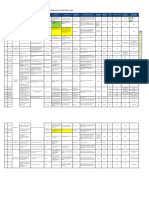
- IH Hospital Wide QI Master Spreadsheet 2023Document115 pagesIH Hospital Wide QI Master Spreadsheet 2023Uranchimeg MyagmarchimedNo ratings yet
- RBC Tests: MCV, MCH, MCHC, RDW, Polycythemia, AnemiaDocument11 pagesRBC Tests: MCV, MCH, MCHC, RDW, Polycythemia, AnemiaDingdongLopezNo ratings yet
- Diagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newDocument94 pagesDiagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newmatrix_oriNo ratings yet
- ModifiedPrinciplesofHaematologyLabManual Fall2016 PDFDocument59 pagesModifiedPrinciplesofHaematologyLabManual Fall2016 PDFGwenNo ratings yet
- Synovial Fluid and Fecal Analysis .Group 5Document39 pagesSynovial Fluid and Fecal Analysis .Group 5John Alfrey Dondiego PuebloNo ratings yet
- WBC BasicsDocument70 pagesWBC BasicsZoe ZillaNo ratings yet
- RBC Count Using HemocytometerDocument4 pagesRBC Count Using Hemocytometermuneebanjum0% (1)
- CAP Presentation On StatisticDocument88 pagesCAP Presentation On StatisticAmirul AriffNo ratings yet
- CSMLS Exam Guide Notes (Referrence Range)Document4 pagesCSMLS Exam Guide Notes (Referrence Range)software4us.2023No ratings yet
- Urine CrystallDocument4 pagesUrine Crystallpartho1432513No ratings yet
- Hematopoietic SystemDocument39 pagesHematopoietic SystemapplesncoreNo ratings yet
- Laboratory Sample Reception EssentialsDocument25 pagesLaboratory Sample Reception EssentialsAngel joyce ValenciaNo ratings yet
- Plasma ProteinsDocument23 pagesPlasma ProteinsNgonie Dube100% (1)
- Hemocytometer ProtocolDocument1 pageHemocytometer ProtocolBiolab ProtocolsNo ratings yet
- CLIAbrochure8 PDFDocument12 pagesCLIAbrochure8 PDFAlexandr Chuvakov100% (1)
- Types of AgarDocument12 pagesTypes of AgarRoyle LolingNo ratings yet
- Coag Made EasyDocument16 pagesCoag Made EasyBrian RobertsNo ratings yet
- The Importance of Considering Thalassaemia in Low MCV or MCH Blood CountsDocument40 pagesThe Importance of Considering Thalassaemia in Low MCV or MCH Blood CountsHenni Junita Siregar SorminNo ratings yet
- Lab Practical UrinalysisDocument7 pagesLab Practical UrinalysisHeatherIz AwwsomeNo ratings yet
- Blood SmearsDocument4 pagesBlood SmearsAmor KourdouliNo ratings yet
- WHO Guidelines On Drawing BloodDocument125 pagesWHO Guidelines On Drawing BloodAnonymous brvvLxoIlu100% (1)
- Clinical Microscopy - MTDocument200 pagesClinical Microscopy - MTJihrus MendozaNo ratings yet
- Isolation and Identification of Enteric OrganismsDocument7 pagesIsolation and Identification of Enteric OrganismsCzarina Charmaine DiwaNo ratings yet
- Gram Positive & Gram Negative Cocci Infections (Staphylococcus, Streptococcus, NeisseriaDocument33 pagesGram Positive & Gram Negative Cocci Infections (Staphylococcus, Streptococcus, NeisseriaRebeka Costantina Weriditi0% (1)
- Hem311 Week 13 Lab - Reticulocyte CountDocument32 pagesHem311 Week 13 Lab - Reticulocyte CountSheine EspinoNo ratings yet
- 29th ChapDocument129 pages29th ChapJoshNo ratings yet
- CSF and Synovial FluidDocument12 pagesCSF and Synovial Fluidquerokeropi100% (1)
- Staphylococcus LectureDocument66 pagesStaphylococcus LectureFarhan Azmain FahimNo ratings yet
- PCV and EsrDocument40 pagesPCV and EsrArslan Arshad100% (2)
- Quality Control2Document32 pagesQuality Control2Mustafa KhandgawiNo ratings yet
- Coagulation NotesDocument14 pagesCoagulation NotesthrowawyNo ratings yet
- WBC MorphologyDocument10 pagesWBC MorphologyGlucose DRglucoseNo ratings yet
- Urinalysis textbook chapters 1-8 safety quality introduction renal function physical chemical microscopic diseases screening metabolic disordersDocument101 pagesUrinalysis textbook chapters 1-8 safety quality introduction renal function physical chemical microscopic diseases screening metabolic disordersDF DasallaNo ratings yet
- Basic Haematology Exercise 1 (MKEB2403)Document10 pagesBasic Haematology Exercise 1 (MKEB2403)kiedd_04100% (8)
- CBCDocument12 pagesCBCDaNa Al-jomah100% (1)
- Glucose Tolerance TestDocument11 pagesGlucose Tolerance TestDharmikPatelNo ratings yet
- Identification of Normal and Abnormal Forms of RedDocument32 pagesIdentification of Normal and Abnormal Forms of RedNada hasanNo ratings yet
- Ana IfDocument101 pagesAna Ifshrikrishnapathlab100% (1)
- Clinical Microscopy Lecture: Chemical Examination of UrineDocument50 pagesClinical Microscopy Lecture: Chemical Examination of UrineThea MallariNo ratings yet
- Understanding CBCDocument9 pagesUnderstanding CBCbettsaltaNo ratings yet
- Blood Morphometry or Blood Film CommentDocument103 pagesBlood Morphometry or Blood Film CommentYangnuu TitusNo ratings yet
- Enterobacteriaceae Identification GuideDocument105 pagesEnterobacteriaceae Identification GuideYelsin Denis Fabian AmbrosioNo ratings yet
- Red Cell and White Cell Counting, BloodDocument89 pagesRed Cell and White Cell Counting, BloodJovel GangcuangcoNo ratings yet
- Clia & Cap Regulatory TrainingDocument23 pagesClia & Cap Regulatory TrainingWilliam David HommelNo ratings yet
- Hematological Investigation or Quantitative Evaluation of The Hematopoietic SystemDocument21 pagesHematological Investigation or Quantitative Evaluation of The Hematopoietic SystemMAMA LALANo ratings yet
- Critical Value in HematologyDocument8 pagesCritical Value in HematologySTARK DIAGNOSTICSNo ratings yet
- Red Blood Cell Morphology: A Seminar on RBC AbnormalitiesDocument11 pagesRed Blood Cell Morphology: A Seminar on RBC AbnormalitiesChabNo ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- Chapter 4 - Hematological MalignanciesDocument99 pagesChapter 4 - Hematological MalignanciesAemro TadeleNo ratings yet
- Chapter 4 - Hematological MalignanciesDocument99 pagesChapter 4 - Hematological MalignanciesAemro TadeleNo ratings yet
- FDocument1 pageFExer CelimaNo ratings yet
- Ethiopian Food and Drug Authority: July 2021 Addis Ababa, EthiopiaDocument23 pagesEthiopian Food and Drug Authority: July 2021 Addis Ababa, EthiopiabiniamNo ratings yet
- Allergic RhinitisDocument27 pagesAllergic Rhinitispaningbatan.kristine.bNo ratings yet
- DHO Chapter 1Document2 pagesDHO Chapter 1Victoria SosaNo ratings yet
- Early-Onset Sepsis in Newborns 2023Document9 pagesEarly-Onset Sepsis in Newborns 2023Charlie CharcapeNo ratings yet
- HFMD Parent Orientation Narrative ReportDocument7 pagesHFMD Parent Orientation Narrative ReportGerald CiudadNo ratings yet
- Acr-Nasci-Sir-Spr Practice Parameter For The Performance and Interpretation of Body Computed Tomography Angiography (Cta)Document15 pagesAcr-Nasci-Sir-Spr Practice Parameter For The Performance and Interpretation of Body Computed Tomography Angiography (Cta)kirim mammoNo ratings yet
- Grandes Desafios para A Prevenção e Reabilitação de Lesões EsportivasDocument5 pagesGrandes Desafios para A Prevenção e Reabilitação de Lesões EsportivasEdilis FlorNo ratings yet
- BurtonFreeman Reimers2011Document12 pagesBurtonFreeman Reimers2011Della FitriaNo ratings yet
- Tiket Juragan GombalDocument3 pagesTiket Juragan Gombaldhebys suryaniNo ratings yet
- Automated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsDocument32 pagesAutomated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsLuis Martínez RamírezNo ratings yet
- Septicemia PresentationDocument23 pagesSepticemia Presentationapi-548307464No ratings yet
- 19 04 2020 Mumbai PDFDocument33 pages19 04 2020 Mumbai PDFShaji VkNo ratings yet
- Clinical NeurologyDocument288 pagesClinical NeurologyWeronika Tomaszczuk-KłakNo ratings yet
- Joseph Murphy Book ReviewsDocument54 pagesJoseph Murphy Book ReviewsDr. Peter Fritz Walter100% (4)
- Cognitive Behavioral Therapy ForDocument7 pagesCognitive Behavioral Therapy Forsyarifah husnaNo ratings yet
- The Importance of Proper Body Mechanics - Keeping Your Spine HealthyDocument25 pagesThe Importance of Proper Body Mechanics - Keeping Your Spine HealthyCristine PraycoNo ratings yet
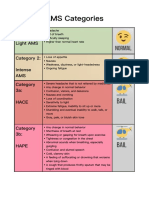
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- © 2017 Lanternfish ESL @Document5 pages© 2017 Lanternfish ESL @DanniNo ratings yet
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- Guia para El Manejo de La Anemia Por Deficiencia de Hierro 2017Document9 pagesGuia para El Manejo de La Anemia Por Deficiencia de Hierro 2017Walther YepesNo ratings yet
- Gardner 2015Document6 pagesGardner 2015Alvaro Quincho LópezNo ratings yet
- Eotc Camp Permission Form PDFDocument3 pagesEotc Camp Permission Form PDFapi-238963120No ratings yet
- A008 MicroVue C4d EnglishDocument15 pagesA008 MicroVue C4d EnglishAlisNo ratings yet
- RV InfarctDocument2 pagesRV Infarctintrovoyz041No ratings yet
- Health PPT 33Document26 pagesHealth PPT 33Kamlesh KumarNo ratings yet
- Antibiotic Resistance Genes in BacteriaDocument22 pagesAntibiotic Resistance Genes in BacteriaGabriel TrevisanNo ratings yet
- Cardiovascular System PharmacothDocument78 pagesCardiovascular System PharmacothKumera Dinkisa ToleraNo ratings yet
- One Shot Revision Patho by DR PraveenDocument19 pagesOne Shot Revision Patho by DR PraveenTauqueer AlamNo ratings yet
- Whole Abdomen (Male)Document48 pagesWhole Abdomen (Male)Eftekharul IslamNo ratings yet
- Kaminsky 2003Document6 pagesKaminsky 2003Gabriel Balbino NogueiraNo ratings yet
- How Do You Know It's TrueDocument36 pagesHow Do You Know It's TrueAANo ratings yet