You might also like
- Basic Mycology For PGIsDocument260 pagesBasic Mycology For PGIsHannah Grace Protasio LumongsodNo ratings yet
- State The Rules or Precautions To Be Observed For Collection of Such SpecimenDocument4 pagesState The Rules or Precautions To Be Observed For Collection of Such SpecimenMarianneTee-ruhNo ratings yet
- Hem311 Week 13 Lab - Reticulocyte CountDocument32 pagesHem311 Week 13 Lab - Reticulocyte CountSheine EspinoNo ratings yet
- Staphylococcus LectureDocument66 pagesStaphylococcus LectureFarhan Azmain FahimNo ratings yet
- Mycology 1 PrelimDocument4 pagesMycology 1 PrelimKaye Angel VillonNo ratings yet
- Lab Practical UrinalysisDocument7 pagesLab Practical UrinalysisHeatherIz AwwsomeNo ratings yet
- Clinical Microscopy Lecture: Chemical Examination of UrineDocument50 pagesClinical Microscopy Lecture: Chemical Examination of UrineThea MallariNo ratings yet
- Archaea and BacteriaDocument20 pagesArchaea and BacteriaLorie Mae Llerin PangandoyonNo ratings yet
- Lab Investigation of AnaemiasDocument109 pagesLab Investigation of AnaemiasMadhura ShekatkarNo ratings yet
- Urinalysis textbook chapters 1-8 safety quality introduction renal function physical chemical microscopic diseases screening metabolic disordersDocument101 pagesUrinalysis textbook chapters 1-8 safety quality introduction renal function physical chemical microscopic diseases screening metabolic disordersDF DasallaNo ratings yet
- RBC Abnormal Morphology GuideDocument33 pagesRBC Abnormal Morphology GuideLailitifa Windy SNo ratings yet
- The Kingdom FungiDocument44 pagesThe Kingdom FungiKunjal100% (30)
- Clinical Microscopy - MTDocument200 pagesClinical Microscopy - MTJihrus MendozaNo ratings yet
- The Insulin Receptor and Mechanism of ActionDocument5 pagesThe Insulin Receptor and Mechanism of ActionMonica AbabeiNo ratings yet
- Selective MediaDocument10 pagesSelective Mediaprincess_likemist4No ratings yet
- Urinalysis and Body Fluids2020Document47 pagesUrinalysis and Body Fluids2020MONFOLA100% (1)
- Viruses PDFDocument54 pagesViruses PDFluz camargoNo ratings yet
- 1 Antigens and AntibodiesDocument31 pages1 Antigens and AntibodiesJohn Louis RanetNo ratings yet
- Staphylococcus Aureus - Pseudomonas Putida - Klebsiella OxytocaDocument4 pagesStaphylococcus Aureus - Pseudomonas Putida - Klebsiella OxytocaJeanette RiosNo ratings yet
- Identification of Normal and Abnormal Forms of RedDocument32 pagesIdentification of Normal and Abnormal Forms of RedNada hasanNo ratings yet
- Blood Film Staining Effects Educational Document PDFDocument5 pagesBlood Film Staining Effects Educational Document PDFCrisiant DolinaNo ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- Week 1 Day 1 LessonDocument143 pagesWeek 1 Day 1 LessonTRIXIE CYRAH MIRANDA SALAVIANo ratings yet
- Vibrio Cholerae Morphology, Culture & PathogenesisDocument85 pagesVibrio Cholerae Morphology, Culture & PathogenesissourabbirlaNo ratings yet
- Bacterial Crowth CurveDocument29 pagesBacterial Crowth CurveDr. Kalavati PrajapatiNo ratings yet
- BIOCHEMICAL TESTING FOR MICROORGANISM IDENTIFICATIONDocument55 pagesBIOCHEMICAL TESTING FOR MICROORGANISM IDENTIFICATIONbujalkanNo ratings yet
- Family Neisseriaceae: Joy P. Calayo, RMT, MSMT UST Faculty of Pharmacy Dept. of Medical TechnologyDocument18 pagesFamily Neisseriaceae: Joy P. Calayo, RMT, MSMT UST Faculty of Pharmacy Dept. of Medical Technologypixholic100% (1)
- Isolation and Identification of Enteric OrganismsDocument7 pagesIsolation and Identification of Enteric OrganismsCzarina Charmaine DiwaNo ratings yet
- ModifiedPrinciplesofHaematologyLabManual Fall2016 PDFDocument59 pagesModifiedPrinciplesofHaematologyLabManual Fall2016 PDFGwenNo ratings yet
- Lecture 11 SCI 8007SEF Medical Microbiology & Virology Topic 5 - Introduction of Mycology - 12 Nov 2023Document80 pagesLecture 11 SCI 8007SEF Medical Microbiology & Virology Topic 5 - Introduction of Mycology - 12 Nov 2023YY CheungNo ratings yet
- Pre-Analytical Considerations in PhlebotomyDocument56 pagesPre-Analytical Considerations in PhlebotomyAngel joyce ValenciaNo ratings yet
- Hemocytometer ProtocolDocument1 pageHemocytometer ProtocolBiolab ProtocolsNo ratings yet
- Microbial Growth Factors and PhasesDocument96 pagesMicrobial Growth Factors and PhasesJenniferNo ratings yet
- Type 3 DiabetesDocument7 pagesType 3 DiabetesAniqua sajidNo ratings yet
- Foundations in Microbiology: Nonspecific Host Defenses TalaroDocument35 pagesFoundations in Microbiology: Nonspecific Host Defenses TalaroOdurNo ratings yet
- DLL Biotechnology - Dec. 2-6,2019Document3 pagesDLL Biotechnology - Dec. 2-6,2019MichaelAbdonDomingoFavo50% (2)
- Lesson 3Document71 pagesLesson 3Angel joyce ValenciaNo ratings yet
- Preventing and Reversing Cancer - The Absolute Health Integrative Oncology MethodDocument56 pagesPreventing and Reversing Cancer - The Absolute Health Integrative Oncology MethodHalal Media MalaysiaNo ratings yet
- Urinalysis 1: Mr. Arian Ray E. MalintadDocument55 pagesUrinalysis 1: Mr. Arian Ray E. MalintadAbraham DemeterioNo ratings yet
- Urinalysis Cases (Revised)Document3 pagesUrinalysis Cases (Revised)Gold NajmNo ratings yet
- Blood SmearsDocument4 pagesBlood SmearsAmor KourdouliNo ratings yet
- Urine CrystallDocument4 pagesUrine Crystallpartho1432513No ratings yet
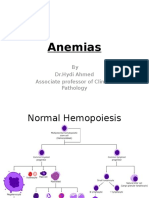
- Anemias (1) by DR - Hydi 3rd MBBS-2016Document63 pagesAnemias (1) by DR - Hydi 3rd MBBS-2016Suban GouseNo ratings yet
- Synovial Fluid and Fecal Analysis .Group 5Document39 pagesSynovial Fluid and Fecal Analysis .Group 5John Alfrey Dondiego PuebloNo ratings yet
- Chapter Two Anemiarev - ATDocument153 pagesChapter Two Anemiarev - ATAemro TadeleNo ratings yet
- Screening Hbpathies 2012Document15 pagesScreening Hbpathies 2012Fiky setiawanNo ratings yet
- Inherited Overflow Metabolic Overflow RenalDocument11 pagesInherited Overflow Metabolic Overflow RenalChrissa Mae Tumaliuan CatindoyNo ratings yet
- CH 6 Part 1Document7 pagesCH 6 Part 1ArenNo ratings yet
- CSF and Synovial FluidDocument12 pagesCSF and Synovial Fluidquerokeropi100% (1)
- Basic Haematology Exercise 1 (MKEB2403)Document10 pagesBasic Haematology Exercise 1 (MKEB2403)kiedd_04100% (8)
- Aubf Prelim 1Document59 pagesAubf Prelim 1Kat JornadalNo ratings yet
- Synovial FluidDocument8 pagesSynovial FluidMary ChristelleNo ratings yet
- Lecture 10 - Urine SedimentsDocument224 pagesLecture 10 - Urine Sedimentsdamaliso nyirongo2No ratings yet
- Hematology 2 Lesson 1Document9 pagesHematology 2 Lesson 1janNo ratings yet
- Chapter 2 Introduction To Urinalysis PDFDocument4 pagesChapter 2 Introduction To Urinalysis PDFJulie Anne Soro ValdezNo ratings yet
- Prelims Week 3 - Urinalysis - TransDocument16 pagesPrelims Week 3 - Urinalysis - TransLoro JDNo ratings yet
- Laboratory Sample Reception EssentialsDocument25 pagesLaboratory Sample Reception EssentialsAngel joyce ValenciaNo ratings yet
- Diagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newDocument94 pagesDiagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newmatrix_oriNo ratings yet
- WBC MorphologyDocument10 pagesWBC MorphologyGlucose DRglucoseNo ratings yet
- Topic 02 Urinalysis I Review of Ana and Phy of KidneysDocument6 pagesTopic 02 Urinalysis I Review of Ana and Phy of KidneysNatasha MendozaNo ratings yet
- Routine UrinalysisDocument74 pagesRoutine UrinalysisGARON KlarizzaNo ratings yet
- Red Cell and White Cell Counting, BloodDocument89 pagesRed Cell and White Cell Counting, BloodJovel GangcuangcoNo ratings yet
- Lecture 2 MLTDocument24 pagesLecture 2 MLTAbood dot netNo ratings yet
- Competent Cell Preparation and TransformationDocument5 pagesCompetent Cell Preparation and TransformationswaroopsanketNo ratings yet
- Brochure Endoshaft - IT-En Rev01Document2 pagesBrochure Endoshaft - IT-En Rev01Marcello RighiniNo ratings yet
- Histology of The Circulatory SystemDocument24 pagesHistology of The Circulatory SystemFatima Zehra YusefNo ratings yet
- Science Alive - Group 4 - Louisa Choi Ambrose Leung Karen Lee Patrick Gale Clancy SteainsDocument23 pagesScience Alive - Group 4 - Louisa Choi Ambrose Leung Karen Lee Patrick Gale Clancy Steainsapi-347649201No ratings yet
- 9.2 Packet Heaven WalkerDocument5 pages9.2 Packet Heaven WalkerHNo ratings yet
- General Biology 2 Quarter 3 Week 1Document9 pagesGeneral Biology 2 Quarter 3 Week 1Leizl GulleNo ratings yet
- A Non Beta Cell Tumor Located in The Abdomen of A Patient With Hypoglycaemia Secreting High Levels of "Big" Insulin-Like Growth Factor (IGF) - II and IGF-binding Protein-6.Document8 pagesA Non Beta Cell Tumor Located in The Abdomen of A Patient With Hypoglycaemia Secreting High Levels of "Big" Insulin-Like Growth Factor (IGF) - II and IGF-binding Protein-6.Wouter van de HoefNo ratings yet
- Journal Presentation Metabolomics and Prakruthi AnalysisDocument17 pagesJournal Presentation Metabolomics and Prakruthi AnalysisDeepa RajaramNo ratings yet
- Goljan Audio TranscriptsDocument201 pagesGoljan Audio Transcriptsendocrinology101No ratings yet
- Biology Form 4 Chapter 4.5 EnzymesDocument11 pagesBiology Form 4 Chapter 4.5 EnzymesSatpal SinghNo ratings yet
- Immunocompromise State in Pregnancy 2013Document51 pagesImmunocompromise State in Pregnancy 2013Suhazeli Abdullah100% (1)
- n094 NeuroscienceDocument74 pagesn094 NeuroscienceAnnaNo ratings yet
- Cellular Energy TransactionsDocument3 pagesCellular Energy TransactionsDrAmit VermaNo ratings yet
- PathologyDocument11 pagesPathologymrcopy xeroxNo ratings yet
- Cell Division AssessmentDocument12 pagesCell Division AssessmentAzween SabtuNo ratings yet
- Biological CommunitiesDocument9 pagesBiological CommunitiesRhodelyn TolentinoNo ratings yet
- Cell DisruptionDocument7 pagesCell DisruptionSamir ChavanNo ratings yet
- Human MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyDocument34 pagesHuman MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyJános JuhászNo ratings yet
- Benefits of Artichoke Leaf ExtractDocument13 pagesBenefits of Artichoke Leaf ExtractFajar RamadhanNo ratings yet
- Meiosis and Tetrad AnalysisDocument10 pagesMeiosis and Tetrad Analysishuangc17No ratings yet
- Twelve Taxa Fissidens Hedw. (Fissidentaceae, Dicranales, Bryopsida) New Distributional Records To Andhra PradeshDocument9 pagesTwelve Taxa Fissidens Hedw. (Fissidentaceae, Dicranales, Bryopsida) New Distributional Records To Andhra PradeshANANTANENI SREENATHNo ratings yet
- S.Y.B.Sc. Zoology 28-12-11Document16 pagesS.Y.B.Sc. Zoology 28-12-11Anooja AnilNo ratings yet
- 14 Ways Plants Benefit Humans & EarthDocument6 pages14 Ways Plants Benefit Humans & EarthdeepakatoliaNo ratings yet
- The Impact of Microbes On The Environment and Human Activities LDocument11 pagesThe Impact of Microbes On The Environment and Human Activities LWulandari SaputriNo ratings yet
- Biochemical EngineeringDocument28 pagesBiochemical Engineeringsurajagtap010% (1)