You might also like
- Notes on Diseases of Cattle: Cause, Symptoms and TreatmentFrom EverandNotes on Diseases of Cattle: Cause, Symptoms and TreatmentNo ratings yet
- Parasitos Oportunistas: Catalina Tovar Acero Msc. Infecciones Y Salud en El TropicalDocument22 pagesParasitos Oportunistas: Catalina Tovar Acero Msc. Infecciones Y Salud en El TropicalAndrés ArrietaNo ratings yet
- Parasitology: - IntroductionDocument62 pagesParasitology: - IntroductionHana AliNo ratings yet
- Giardia Presen... NotesDocument75 pagesGiardia Presen... Notestheintrov100% (1)
- 2 VPAR-55 Lec DicrocoeliidaeDocument25 pages2 VPAR-55 Lec DicrocoeliidaeLOUISE ANNE NAGALNo ratings yet
- Flagellates. Applied Parasitology & MycologyDocument34 pagesFlagellates. Applied Parasitology & MycologyRaunaNo ratings yet
- Ascaris Lumbricoides: Giant Intestinal RoundwormDocument63 pagesAscaris Lumbricoides: Giant Intestinal RoundwormidelviceNo ratings yet
- Ascaris LEM 2022Document36 pagesAscaris LEM 2022Kenny NgowiNo ratings yet
- Parasitology: Is The Study of ParasitesDocument51 pagesParasitology: Is The Study of ParasitesMarz ALNo ratings yet
- Giardia PPT M.SC Medical 4th SemDocument16 pagesGiardia PPT M.SC Medical 4th SemRahul ChaudharyNo ratings yet
- Entamoeba Histolytica: Causes: Amoebiasis. Geog - Distribution: Habitat: Infective Stage: Mode of InfectionDocument46 pagesEntamoeba Histolytica: Causes: Amoebiasis. Geog - Distribution: Habitat: Infective Stage: Mode of InfectionAlfia Nikmah100% (3)
- Trematodes: Prepared By: Charriz A. AmoyanDocument48 pagesTrematodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- 3.b.coli, Crypt, Cyclo, Iso, Sarco, Microsp, Acnth, NaegDocument86 pages3.b.coli, Crypt, Cyclo, Iso, Sarco, Microsp, Acnth, NaegPallavi Uday NaikNo ratings yet
- Ascariasis & GiardiasisDocument34 pagesAscariasis & GiardiasisMuhammad ShahzadNo ratings yet
- Schistosomapptdrsomesh2015 151217103710Document39 pagesSchistosomapptdrsomesh2015 151217103710Al Karkab آل كركابNo ratings yet
- Ascaris LumbricoidesDocument24 pagesAscaris LumbricoidesQonik Nuzulul FalakhiNo ratings yet
- Giardia LambliaDocument28 pagesGiardia LambliaMegbaruNo ratings yet
- 8-Trematodes Ibrahim2016Document35 pages8-Trematodes Ibrahim2016Buntukazi MapamelaNo ratings yet
- Protozoology 2 13.11Document58 pagesProtozoology 2 13.11Manav VyasNo ratings yet
- 5.1.3.2. Blood FlukesDocument43 pages5.1.3.2. Blood Flukestadele10100% (1)
- Flagellates: Al-Anbar University College of Medicine Dr. Huda. R. Sabbar B.SC., M. SC., Ph.d. Med - MicrobiologyDocument38 pagesFlagellates: Al-Anbar University College of Medicine Dr. Huda. R. Sabbar B.SC., M. SC., Ph.d. Med - MicrobiologyThunderNo ratings yet
- G. LambliaDocument32 pagesG. Lambliaturinawe haggaiNo ratings yet
- Proto Lec7Document25 pagesProto Lec7Syed Hammad UllahNo ratings yet
- Para2020 10Document46 pagesPara2020 10Koko HashamNo ratings yet
- 01 - Parasitic Infections 2020Document85 pages01 - Parasitic Infections 2020gilbert agudoNo ratings yet
- Parasitology - MTAPDocument278 pagesParasitology - MTAPMarron MonsaludNo ratings yet
- Parasitology Lecture 2Document85 pagesParasitology Lecture 2Dr Sarah Bakhsh - Resident FCPS Community MedicineNo ratings yet
- Schistosomes Parasite in HumanDocument27 pagesSchistosomes Parasite in HumanAnonymous HXLczq3No ratings yet
- Micro ParasitologyDocument5 pagesMicro ParasitologyPlzstudylav SyedNo ratings yet
- AscarisDocument18 pagesAscarisHabib UllahNo ratings yet
- VMP 5265 Parasitology 4. Nematodes - Strongylida Strongyloidea ContDocument40 pagesVMP 5265 Parasitology 4. Nematodes - Strongylida Strongyloidea ContJessica KadykNo ratings yet
- 03 SchistosomesDocument16 pages03 SchistosomesAlvin LaurenceNo ratings yet
- Reported by Ocampo, Eirene Joy Louise N. BSN110Document66 pagesReported by Ocampo, Eirene Joy Louise N. BSN110roy mata100% (1)
- Kuliah 17 - Nematoda Dan ProtozoaDocument72 pagesKuliah 17 - Nematoda Dan ProtozoaivaNo ratings yet
- Medical Helminthology - Chordata and Roundworms - Human ParasitesDocument54 pagesMedical Helminthology - Chordata and Roundworms - Human ParasitesMewa MahartaNo ratings yet
- Trematodes PDFDocument46 pagesTrematodes PDFAsnorah SaripNo ratings yet
- Lecture 11C - Introduction To Worms (Trematodes)Document47 pagesLecture 11C - Introduction To Worms (Trematodes)Nida Ridzuan100% (1)
- Family-Fasciolidae Genus: Fasciola: F. Hepatica, F. GiganticaDocument3 pagesFamily-Fasciolidae Genus: Fasciola: F. Hepatica, F. GiganticaSumit Sharma PoudelNo ratings yet
- NematodesDocument110 pagesNematodesRussel Bob BorromeoNo ratings yet
- Lecture# Food-Borne Virus, Protozoa PrionsDocument40 pagesLecture# Food-Borne Virus, Protozoa PrionsSaravana KumarNo ratings yet
- Group Number 8Document17 pagesGroup Number 8willisonjohn155No ratings yet
- Other Intestinal ProtozoansDocument26 pagesOther Intestinal ProtozoansCharlene SuliganNo ratings yet
- Parasitology Lec 4Document14 pagesParasitology Lec 4ao868598No ratings yet
- GI Protozoal & Infections Caused by HelminthsDocument39 pagesGI Protozoal & Infections Caused by HelminthsSHIHAB UDDIN KAZINo ratings yet
- Cestodes: Prepared By: Charriz A. AmoyanDocument37 pagesCestodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- Schistosoma LectureDocument10 pagesSchistosoma LectureSe YiNo ratings yet
- Communicable and Vector Bone Diseases1) - 1Document175 pagesCommunicable and Vector Bone Diseases1) - 1staceyatienoomaNo ratings yet
- Fasciola HepaticaDocument38 pagesFasciola HepaticaDeni Susanto100% (1)
- Intestinal Coccidian ParasitesDocument23 pagesIntestinal Coccidian ParasitesABC100% (1)
- Giardia Lamblia: The CystDocument30 pagesGiardia Lamblia: The CysterinastevianaNo ratings yet
- Hymenolepis Nana Group 5 Write UpDocument7 pagesHymenolepis Nana Group 5 Write UpSusan GachukiaNo ratings yet
- Screenshot 2024-02-28 at 9.47.36 AMDocument36 pagesScreenshot 2024-02-28 at 9.47.36 AMfftemmmNo ratings yet
- Urinary Tract InfectionDocument9 pagesUrinary Tract InfectionTom Mallinson100% (1)
- AscariasisDocument6 pagesAscariasisPika PearlasNo ratings yet
- 12 - NematodaDocument44 pages12 - NematodaAnnisya MaharaniNo ratings yet
- AmoebaDocument36 pagesAmoebaSarah BirechNo ratings yet
- CestodesDocument70 pagesCestodesBlanche AltheaNo ratings yet
- Intestinal and Genital Flagellates-EditDocument7 pagesIntestinal and Genital Flagellates-EditChristianAvelinoNo ratings yet
- Trematod1 EnglishDocument60 pagesTrematod1 EnglishTara AlmosaNo ratings yet
- Human Blood Trematodes4Document65 pagesHuman Blood Trematodes4Ali WalayNo ratings yet
- 988611457NK448908 Vehicle Scan ReportDocument5 pages988611457NK448908 Vehicle Scan ReportVictor Daniel Piñeros ZubietaNo ratings yet
- Clinical Reviews: The Management of Children With Gastroenteritis and Dehydration in The Emergency DepartmentDocument13 pagesClinical Reviews: The Management of Children With Gastroenteritis and Dehydration in The Emergency DepartmentRina Dewi AnggraeniNo ratings yet
- 2nd APJ Abdul Kalam Essay Writing CompetitionDocument2 pages2nd APJ Abdul Kalam Essay Writing CompetitionANURAG SINGHNo ratings yet
- Smart Grid TechnologyDocument43 pagesSmart Grid Technologyarnav LakshkarNo ratings yet
- Test09 Eoc Algebra2 ReducedDocument33 pagesTest09 Eoc Algebra2 ReducedkristymadimikeNo ratings yet
- Homeo Treatment of Eye Diseases and AllergiesDocument17 pagesHomeo Treatment of Eye Diseases and AllergiesZia AbbasiNo ratings yet
- Colour FastnessDocument37 pagesColour FastnessSivakumar K100% (1)
- 08 - 2061 USTR 2222a (1) Supor EKVDocument24 pages08 - 2061 USTR 2222a (1) Supor EKVHassan Houdoud0% (1)
- Water Filling MachineDocument15 pagesWater Filling Machinepallab D RozarioNo ratings yet
- Kaged Muscle Magazine Issue 1Document41 pagesKaged Muscle Magazine Issue 1hashimhafiz1100% (1)
- DIVAR IP All-In-One 7000 3U Datasheet 51 en 66297110155Document5 pagesDIVAR IP All-In-One 7000 3U Datasheet 51 en 66297110155Javier RochaNo ratings yet
- YoungMan EN131 GUIDEDocument16 pagesYoungMan EN131 GUIDErcpawar100% (1)
- RepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUDocument2 pagesRepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUPR.comNo ratings yet
- Iodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04Document12 pagesIodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04stevgonNo ratings yet
- Gaffin, Biblical Theology and Westminster StandardsDocument16 pagesGaffin, Biblical Theology and Westminster StandardstheoarticlesNo ratings yet
- ARK - Intel® Core™ I3-370m Processor (3M Cache, 2Document3 pagesARK - Intel® Core™ I3-370m Processor (3M Cache, 2Delzi Guindra AdriNo ratings yet
- T.A.T.U. - Waste Management - Digital BookletDocument14 pagesT.A.T.U. - Waste Management - Digital BookletMarieBLNo ratings yet
- The Process: by Andy ZoppeltDocument4 pagesThe Process: by Andy ZoppeltMark Stephen HuBertNo ratings yet
- Hypothesis Testing - IDocument36 pagesHypothesis Testing - Isai revanthNo ratings yet
- FBC MNCS Service-, Error-, Infocodes ENDocument23 pagesFBC MNCS Service-, Error-, Infocodes ENDragos Stoian100% (1)
- Badminton ReviewerDocument10 pagesBadminton ReviewerHailsey WinterNo ratings yet
- 15 Benefits of CyclingDocument8 pages15 Benefits of CyclingJoycs PintoNo ratings yet
- Concrete Super Structure ReportDocument43 pagesConcrete Super Structure ReportLivian TeddyNo ratings yet
- Climbing FormworkDocument4 pagesClimbing FormworkAshwin B S RaoNo ratings yet
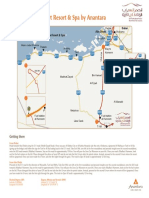
- Qasr Al Sarab Desert Resort Location Map June2012Document1 pageQasr Al Sarab Desert Resort Location Map June2012Anant GârgNo ratings yet
- Exercise On Word Formation 2 (Unit 2 - Advanced) : Tran Dai Nghia High School For The GiftedDocument3 pagesExercise On Word Formation 2 (Unit 2 - Advanced) : Tran Dai Nghia High School For The GiftedEveryonehateshiuzo 2.0No ratings yet
- Tabla9 1Document1 pageTabla9 1everquinNo ratings yet
- Prevailing Torque Locknut Technical SpecificationsDocument3 pagesPrevailing Torque Locknut Technical SpecificationsLiu YangtzeNo ratings yet
- Compiled LecsDocument24 pagesCompiled LecsNur SetsuNo ratings yet
- Nomenclatura SKFDocument1 pageNomenclatura SKFJuan José MeroNo ratings yet