You might also like
- E7 Environment Related InjuriesDocument46 pagesE7 Environment Related InjuriesMuhammad MuaazNo ratings yet
- EnvironmentDocument59 pagesEnvironmentMISBAH NAZNo ratings yet
- Environmental Cold Injury and Illness Prevention PolicyDocument12 pagesEnvironmental Cold Injury and Illness Prevention Policyapi-381026050No ratings yet
- Prentice9e Im Chap07Document7 pagesPrentice9e Im Chap07api-281340024No ratings yet
- Lesson 7 - Hyperthermia and HypothermiaDocument6 pagesLesson 7 - Hyperthermia and HypothermiaArgie BatiancilaNo ratings yet
- Heat StressDocument29 pagesHeat StressAmeenudeenNo ratings yet
- Environmental Emergencies ParamedicDocument90 pagesEnvironmental Emergencies ParamedicPaulhotvw67100% (2)
- Heat Stress Prevention GuideDocument5 pagesHeat Stress Prevention GuidenoormuddassirkhanNo ratings yet
- Heat Stress Plan 01Document13 pagesHeat Stress Plan 01ramod100% (1)
- Cold Weather Risks Can Be Reduced - enDocument1 pageCold Weather Risks Can Be Reduced - enMarwan MalekNo ratings yet
- PNTC Colleges: Senior High SchoolDocument7 pagesPNTC Colleges: Senior High SchoolRodolfo CalindongNo ratings yet
- WORKING IN COLD GUIDELINESDocument8 pagesWORKING IN COLD GUIDELINESasimnaqvi2008No ratings yet
- PRINCIPLES OF ENVIRONMENTAL DISEASESDocument27 pagesPRINCIPLES OF ENVIRONMENTAL DISEASESSHIHAB UDDIN KAZINo ratings yet
- 5.paparan PanasDocument36 pages5.paparan PanasMarta Juwita SitumorangNo ratings yet
- Heat Stress Management ProcedureDocument7 pagesHeat Stress Management ProcedureSameer M. TalibNo ratings yet
- Report On HeatDocument3 pagesReport On HeatKirbey TecsonNo ratings yet
- Safety Etiquettes and Community ResourcesDocument35 pagesSafety Etiquettes and Community ResourcesFundae DesignsNo ratings yet
- Heat Stress Prevention TipsDocument3 pagesHeat Stress Prevention TipsLawrence adeleke OmisakinNo ratings yet
- 2011 - 06 - 10 - Ehs AlertDocument2 pages2011 - 06 - 10 - Ehs Alertpunitg_2No ratings yet
- PEH4-5-ADocument4 pagesPEH4-5-Awilmer.directoNo ratings yet
- DM-PH&SD-P4-TG03 - (Guidelines For Heat Stress at Work)Document3 pagesDM-PH&SD-P4-TG03 - (Guidelines For Heat Stress at Work)kevin100% (1)
- SITE HEAT STRESS PREVENTIONDocument14 pagesSITE HEAT STRESS PREVENTIONCasenillo JovaniNo ratings yet
- Environmental EmergenciesDocument38 pagesEnvironmental EmergenciesIshaBrijeshSharmaNo ratings yet
- Assessment and Management of HypothermiaDocument20 pagesAssessment and Management of HypothermiaJaphter MoongaNo ratings yet
- Assignment 2 - Group Assignment - Injury in The EnivronmentDocument9 pagesAssignment 2 - Group Assignment - Injury in The EnivronmentDezéreaNo ratings yet
- Environmental Emergencies Heat Exhaustion HeatstrokeDocument6 pagesEnvironmental Emergencies Heat Exhaustion HeatstrokepauchanmnlNo ratings yet
- Provide gentle care and warmth. Monitor breathing and pulse. If necessary, provide CPR.5. Monitor breathing and pulse. Provide CPR if necessaryDocument25 pagesProvide gentle care and warmth. Monitor breathing and pulse. If necessary, provide CPR.5. Monitor breathing and pulse. Provide CPR if necessaryNova Kristine MaglupayNo ratings yet
- Dealing With Heat StressDocument11 pagesDealing With Heat StressIlyes FerenczNo ratings yet
- Heat Wave Impact on HealthDocument40 pagesHeat Wave Impact on HealthRaghu Rajan100% (1)
- NCM 106 Care of Client with Heat Stroke and ExhaustionDocument2 pagesNCM 106 Care of Client with Heat Stroke and ExhaustionshydlNo ratings yet
- Heat StrokeDocument2 pagesHeat StrokeshydlNo ratings yet
- Gta08 05 060Document2 pagesGta08 05 060PATRIOTSKULLZNo ratings yet
- heat-sample-programDocument6 pagesheat-sample-programSaurabh SinghNo ratings yet
- FF REHAB Medical MontoringDocument124 pagesFF REHAB Medical MontoringJosh MartinNo ratings yet
- Jurnal Heat DisorderDocument8 pagesJurnal Heat DisorderDiatri Eka DentaNo ratings yet
- Heat Stroke: Heatstroke Signs and Symptoms IncludeDocument5 pagesHeat Stroke: Heatstroke Signs and Symptoms IncludeTomNo ratings yet
- REFLECTION PE & HealthDocument1 pageREFLECTION PE & HealthPenelope CarandangNo ratings yet
- Heat StrokeDocument22 pagesHeat StrokeCrizza Maglasang100% (1)
- Heat Stress: Tailgate Topic March Week 1Document13 pagesHeat Stress: Tailgate Topic March Week 1perezesNo ratings yet
- Heat Related Disorders Abstract PDFDocument4 pagesHeat Related Disorders Abstract PDFEnida XhaferiNo ratings yet
- Heat Related Disorders AbstractDocument4 pagesHeat Related Disorders AbstractEnida XhaferiNo ratings yet
- Physiology of Heat Illnesses and FeverDocument12 pagesPhysiology of Heat Illnesses and FeverKusuma Edhi KuncoroNo ratings yet
- 12CHDocument5 pages12CHTeum Gilliam DbaNo ratings yet
- The Objectives of Applying First Aid in Every Emergency Situation AreDocument27 pagesThe Objectives of Applying First Aid in Every Emergency Situation AreShekinah May Solano AgsawayNo ratings yet
- HypothermiaDocument4 pagesHypothermiaNisa NurimaniahSasmitaNo ratings yet
- Heat Stress EZ EXPLANATIONDocument9 pagesHeat Stress EZ EXPLANATIONsai ganeshNo ratings yet
- What is heat strokeDocument2 pagesWhat is heat strokeTomas Cordia CornelioNo ratings yet
- Al Khandamah SS Heat Illness Prevention and Emergency Response Report 12 May 2018Document18 pagesAl Khandamah SS Heat Illness Prevention and Emergency Response Report 12 May 2018Zaheer AhmedNo ratings yet
- q2 w1 Sports First AidDocument4 pagesq2 w1 Sports First AidLucky G. RupersoNo ratings yet
- First Aid Safety Meeting TopicsDocument79 pagesFirst Aid Safety Meeting TopicsSrikanth BammhideNo ratings yet
- Heat Stress PreventionDocument26 pagesHeat Stress PreventionSameer OmarNo ratings yet
- FrostbiteDocument17 pagesFrostbiteIsabel Barredo Del Mundo100% (2)
- Working in The ColdDocument37 pagesWorking in The ColdBarry MurphyNo ratings yet
- PE-FINALSDocument4 pagesPE-FINALSMhonabelle SalomonNo ratings yet
- Physical Activity Safety ProtocolDocument2 pagesPhysical Activity Safety ProtocolIan M. DimanalataNo ratings yet
- FrostbiteDocument13 pagesFrostbiteRosalyn YuNo ratings yet
- Diagnosis and Management of Heatstroke: I Gede Yasa AsmaraDocument8 pagesDiagnosis and Management of Heatstroke: I Gede Yasa AsmaraputryaNo ratings yet
- Nur 111 Session 21 Sas 1Document8 pagesNur 111 Session 21 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Hypothermia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypothermia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Nanotech MedDocument12 pagesNanotech MedDaphane Kate AureadaNo ratings yet
- Urine screening for metabolic disordersDocument23 pagesUrine screening for metabolic disordersFrances FranciscoNo ratings yet
- Kelsey Camangian: August 2019 - PresentDocument1 pageKelsey Camangian: August 2019 - Presentapi-583563266No ratings yet
- 2018-09-01 Men's Fitness UK PDFDocument116 pages2018-09-01 Men's Fitness UK PDFsalik salmanNo ratings yet
- Four Scenarios for the Future of BioSciences Report HighlightsDocument8 pagesFour Scenarios for the Future of BioSciences Report HighlightsTejaNo ratings yet
- Pre-Intermediate/Intermediate Reading Text: LongevityDocument2 pagesPre-Intermediate/Intermediate Reading Text: LongevityMaria Vitória Carvalho100% (1)
- 10 Science Imp Ch8 1Document8 pages10 Science Imp Ch8 1Rohan SenapathiNo ratings yet
- Ophthalmology Review Manual 2nd EditionDocument538 pagesOphthalmology Review Manual 2nd EditionAnonymous 4OnqyBErNo ratings yet
- Treatment For Spider Veins On LegsDocument3 pagesTreatment For Spider Veins On LegsZackNo ratings yet
- IOC Investors' Report Final 16 Aug 2019Document21 pagesIOC Investors' Report Final 16 Aug 2019Amri Satria NugrahaNo ratings yet
- Quiz BiochemistryDocument100 pagesQuiz BiochemistryMedShare88% (25)
- Sample of Journal & Critique PresenationDocument42 pagesSample of Journal & Critique PresenationMonika shankarNo ratings yet
- LEAK REPAIR PROGRAMSDocument2 pagesLEAK REPAIR PROGRAMSPradip GuptaNo ratings yet
- WGI Benefit GuideDocument32 pagesWGI Benefit GuideSlim ShadyNo ratings yet
- Analysis of Survival Data - LN - D Zhang - 05Document264 pagesAnalysis of Survival Data - LN - D Zhang - 05mirceacomanro2740100% (1)
- Kirk D. Strosahl PHD, Patricia J. Robinson PHD - in This Moment - Five Steps To Transcending Stress Using Mindfulness and Neuroscience (2015, New Harbinger Publications)Document133 pagesKirk D. Strosahl PHD, Patricia J. Robinson PHD - in This Moment - Five Steps To Transcending Stress Using Mindfulness and Neuroscience (2015, New Harbinger Publications)Fábio Vacaro CulauNo ratings yet
- Golden Shield BrochureDocument11 pagesGolden Shield BrochureRak Esh RakeshNo ratings yet
- Document - Isk ..Document8 pagesDocument - Isk ..Karyn GloriaNo ratings yet
- Research PaperDocument27 pagesResearch PaperAngela Grace Dave0% (2)
- TonsilitisDocument23 pagesTonsilitisCrisantaMadrid0% (1)
- Maharashtra PG Medical Entrance Review CorrectionsDocument38 pagesMaharashtra PG Medical Entrance Review Correctionsklingon45No ratings yet
- Trap Cropping-Valuable Pest ManagementDocument4 pagesTrap Cropping-Valuable Pest ManagementmramagroNo ratings yet
- TLE-HE (Dressmaking) : Activity Sheet Quarter 0 - MELC 4Document15 pagesTLE-HE (Dressmaking) : Activity Sheet Quarter 0 - MELC 4Mari PagxNo ratings yet
- Gram Positive Cocci Bacteriology ChartDocument2 pagesGram Positive Cocci Bacteriology ChartIsabella CeaNo ratings yet
- Ecc Class 122 Pediatric McqsDocument44 pagesEcc Class 122 Pediatric McqsDinabandhu BaradNo ratings yet
- English practice test with 20 questionsDocument23 pagesEnglish practice test with 20 questionsHà ChiNo ratings yet
- Frozen Fresh Food As One of The Solutions To Help Isolated Victims of Disaster Get Healthy FoodDocument52 pagesFrozen Fresh Food As One of The Solutions To Help Isolated Victims of Disaster Get Healthy FoodB1Riansyah FakhiratunnisaNo ratings yet
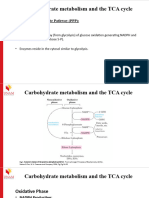
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- Fast F A S T: Recognizing Stroke: Ace Rms Peech ImeDocument25 pagesFast F A S T: Recognizing Stroke: Ace Rms Peech ImeIliescu DenisaNo ratings yet
- Discuss Thoracic IncisionsDocument47 pagesDiscuss Thoracic IncisionsSucipto HartonoNo ratings yet