You might also like
- Endocrine WorksheetDocument7 pagesEndocrine WorksheetBrenda Zaragoza63% (8)
- Assessing The Thorax and LungsDocument3 pagesAssessing The Thorax and LungsZJ GarcianoNo ratings yet
- A. Vertical Strustural Irregularity (NSCP Table 208-9) Type of Irregularity Graphic InterpretationDocument2 pagesA. Vertical Strustural Irregularity (NSCP Table 208-9) Type of Irregularity Graphic InterpretationHarold Roinan Beñabon100% (2)
- Unit 06 Assessment of Thorax and LungDocument55 pagesUnit 06 Assessment of Thorax and Lunghuma100% (1)
- Respiratory AssessmentDocument43 pagesRespiratory AssessmentLui Andrei AnilaNo ratings yet
- Assessment of Respiratory System: Group 3Document33 pagesAssessment of Respiratory System: Group 3ChicieMonalisaNo ratings yet
- Health Assessment Chapter 7 Assessment of Respiratory SystemDocument20 pagesHealth Assessment Chapter 7 Assessment of Respiratory SystemnadyaNo ratings yet
- Pemeriksaan Fisik Sistem Pernapasan: Equipment NeededDocument78 pagesPemeriksaan Fisik Sistem Pernapasan: Equipment Neededsri karinaNo ratings yet
- Thera Pulmo RehabDocument31 pagesThera Pulmo RehabMarcus VictaNo ratings yet
- Assessment of Respiratory SystemDocument18 pagesAssessment of Respiratory SystemIbi Yulia Setyani100% (1)
- Assessment of Respiratory SystemDocument34 pagesAssessment of Respiratory SystemKristal Jade Yanto Esquillo100% (1)
- Topic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Document39 pagesTopic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Ben JilhanoNo ratings yet
- Lecture Respiratory Medicine - Clinical ExaminationDocument39 pagesLecture Respiratory Medicine - Clinical Examinationgloria anyebeNo ratings yet
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla67% (3)
- Examination of Thorax and LungsDocument7 pagesExamination of Thorax and LungsJohanei Mae PeraltaNo ratings yet
- CPAC SON HA 7 Thorax 1Document59 pagesCPAC SON HA 7 Thorax 1misshalieediiNo ratings yet
- UntitledDocument4 pagesUntitledJeizel IgnacioNo ratings yet
- Gnrs 5320 Lessonpowerpoint RevisedDocument30 pagesGnrs 5320 Lessonpowerpoint Revisedapi-277849152No ratings yet
- Respiratory SystemDocument23 pagesRespiratory SystemSaraNo ratings yet
- Assessment Pulmonary ExamDocument3 pagesAssessment Pulmonary Examdd marshallNo ratings yet
- 4 - The Thorax and LungsDocument75 pages4 - The Thorax and LungsXtylish Bacha 8bpNo ratings yet
- Pulmonary Assessment: Components of The AssessmentDocument6 pagesPulmonary Assessment: Components of The AssessmentWenzy Razzie cruzNo ratings yet
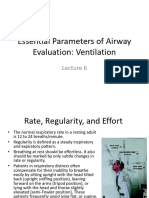
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Chest ExaminationDocument5 pagesChest Examinationalin malekNo ratings yet
- The Thorax and The Lungs: Group 11 FMPDocument27 pagesThe Thorax and The Lungs: Group 11 FMPTisha TancongcoNo ratings yet
- Approach To Child With WheezingpediatricsDocument25 pagesApproach To Child With WheezingpediatricsshahinaNo ratings yet
- Pulmonary Assessment: Components of The AssessmentDocument7 pagesPulmonary Assessment: Components of The Assessmentjoanna gurtizaNo ratings yet
- Respiratorysystem 16Document35 pagesRespiratorysystem 16api-340406981No ratings yet
- Respiratory Assessment 2Document24 pagesRespiratory Assessment 2Kendal BartonNo ratings yet
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- 1.2.4 Lung & RS Exam - SendDocument47 pages1.2.4 Lung & RS Exam - Senddanielndaa51No ratings yet
- Physical ExaminationDocument55 pagesPhysical Examinationdakshpanchal26369No ratings yet
- Respiratory SystemDocument13 pagesRespiratory SystemChristine LeeNo ratings yet
- Respiratory SystemDocument2 pagesRespiratory SystemAnil SathyadasNo ratings yet
- HAPE - Thorax and LungsDocument20 pagesHAPE - Thorax and Lungsaabbccss1.z71No ratings yet
- Publication 2 21768 958Document41 pagesPublication 2 21768 958Safi MohammedNo ratings yet
- NCM 103 - Oxy RespiDocument21 pagesNCM 103 - Oxy RespiMaureen Gonzalo-FlorendoNo ratings yet
- Clinical SkilllllllllllllllDocument12 pagesClinical SkilllllllllllllllAlmira Putri100% (1)
- Week 5 Respiratory System SB Final-محولDocument121 pagesWeek 5 Respiratory System SB Final-محولWalaa 1998No ratings yet
- Physical Assessment Guide THORAX and LUNGSDocument5 pagesPhysical Assessment Guide THORAX and LUNGSJasmine Kate PatenioNo ratings yet
- Nursing Assesment 2019Document17 pagesNursing Assesment 2019Jemmy KherisnaNo ratings yet
- Soal Stridor, Aspiration,&CoughDocument36 pagesSoal Stridor, Aspiration,&CoughWidya AdiartiNo ratings yet
- 14 Assessment of The Throax and LungDocument68 pages14 Assessment of The Throax and LungCruz YrNo ratings yet
- Respiratory System Assessment PDFDocument53 pagesRespiratory System Assessment PDFJay RomeNo ratings yet
- Pemeriksaan Fisik ParuDocument7 pagesPemeriksaan Fisik ParuLila WatiningrumNo ratings yet
- Respiratory Assessment and Treatments: Presented by ATOP Clinical StaffDocument39 pagesRespiratory Assessment and Treatments: Presented by ATOP Clinical StaffNoralyn AsgariNo ratings yet
- SodaPDF Merged Merging ResultDocument648 pagesSodaPDF Merged Merging ResultFaith madayagNo ratings yet
- 2020thoraxlungs Neckheart VesselsDocument171 pages2020thoraxlungs Neckheart VesselsFaith madayagNo ratings yet
- Assessment PDFDocument5 pagesAssessment PDFChris AnnNo ratings yet
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla100% (4)
- SS1 Dma09220034Document5 pagesSS1 Dma09220034alin malekNo ratings yet
- PalpationDocument44 pagesPalpationjenyNo ratings yet
- Respiratory Examination: The Position of The PatientDocument24 pagesRespiratory Examination: The Position of The PatientMuhammed Barznji100% (1)
- Chest Examination: Syeda Afsheen Daud Lecturer IPMR KMUDocument59 pagesChest Examination: Syeda Afsheen Daud Lecturer IPMR KMUCHANGEZ KHAN SARDARNo ratings yet
- Assessing Thorax and LungsDocument26 pagesAssessing Thorax and LungsTarah LedesmaNo ratings yet
- Lungs and ThoraxDocument9 pagesLungs and ThoraxMaria Mika Ella RetizaNo ratings yet
- Objectives of Physical AssessmentDocument10 pagesObjectives of Physical Assessmentemman_abz100% (1)
- Lessons in Artistic Deep Breathing for Strengthening the VoiceFrom EverandLessons in Artistic Deep Breathing for Strengthening the VoiceRating: 5 out of 5 stars5/5 (1)
- FactoringDocument1 pageFactoringGary NugasNo ratings yet
- Text1-Introduction To Cost Accounting-Student ResourceDocument22 pagesText1-Introduction To Cost Accounting-Student Resourcekinai williamNo ratings yet
- Why Some Countries Fail To ThriveDocument23 pagesWhy Some Countries Fail To ThriveSteve B. Salonga100% (2)
- 10.2.2.3 Packet Tracer - Troubleshooting Single-Area OSPFv2 Instructions - ILMDocument2 pages10.2.2.3 Packet Tracer - Troubleshooting Single-Area OSPFv2 Instructions - ILMSergio TejedorNo ratings yet
- Green Fingers Organic FarmsDocument17 pagesGreen Fingers Organic FarmsajdeclandNo ratings yet
- The Complete Series V FINAL PDFDocument227 pagesThe Complete Series V FINAL PDFFabian Villota100% (6)
- Types of Juicers - EditedDocument17 pagesTypes of Juicers - EditedAbdulrehmanNo ratings yet
- XIS-100X: Mid-Sized High Performance SystemDocument2 pagesXIS-100X: Mid-Sized High Performance SystemTalal abou abdallahNo ratings yet
- IGCSE Edexcel CircuitsDocument87 pagesIGCSE Edexcel CircuitsКіра Струлєва ОлексіївнаNo ratings yet
- Sika Guard Water Repealant (Internal Coating)Document2 pagesSika Guard Water Repealant (Internal Coating)anon_429095396No ratings yet
- Gram PositiveDocument14 pagesGram PositiveMiguel Adrian GaonaNo ratings yet
- Manual VSD Ls Ig5aDocument109 pagesManual VSD Ls Ig5arochimunNo ratings yet
- Dolphs Varnishs Resin ChartDocument3 pagesDolphs Varnishs Resin ChartFernando Rodriguez100% (1)
- ReadingDocument2 pagesReadingadriana guerreroNo ratings yet
- UNIT - I Wave Mechanics - Nmamit 2019-20Document50 pagesUNIT - I Wave Mechanics - Nmamit 2019-20Mr.Manjunath K.B NMAMIT PhysicsNo ratings yet
- DEP 31.40.60.11-Gen. Rev. Sep 2002Document19 pagesDEP 31.40.60.11-Gen. Rev. Sep 2002Subbu AbuNo ratings yet
- Trans-Boundary Fisheries Resources Management (Compatibility Mode)Document16 pagesTrans-Boundary Fisheries Resources Management (Compatibility Mode)KruNont MatchPointNo ratings yet
- Battery Charger Series: PowerbaseDocument1 pageBattery Charger Series: PowerbaseCristopher Jason Lopez CansinoNo ratings yet
- ScriptDocument11 pagesScriptmehnoor kaurNo ratings yet
- Lecture 3 Bilinear TFDocument32 pagesLecture 3 Bilinear TFNathan KingoriNo ratings yet
- The Splicing Handbook Chapter 1Document17 pagesThe Splicing Handbook Chapter 1Archie AdkinsNo ratings yet
- NW June P1 2019 MemoDocument6 pagesNW June P1 2019 MemoAsandaNo ratings yet
- DocumentDocument4 pagesDocumentRoque RkhennNo ratings yet
- IDIN-3 DTV3 Extra Grammar Exercises I PARTIALDocument4 pagesIDIN-3 DTV3 Extra Grammar Exercises I PARTIALrobert martinezNo ratings yet
- TNCTDocument2 pagesTNCTjeffrey c. aguilarNo ratings yet
- Respironics WhisperFlow CPAP - User ManualDocument24 pagesRespironics WhisperFlow CPAP - User ManualJoão Francisco MontanhaniNo ratings yet
- Fittings HoseDocument40 pagesFittings HoseSeif HabbachiNo ratings yet
- Apple Rust DiseasesDocument5 pagesApple Rust DiseasesJames ManriqueNo ratings yet