You might also like
- Pharmacognosy Chapter 9 Herbs As Health Food NotesDocument12 pagesPharmacognosy Chapter 9 Herbs As Health Food NotesAbhishek palNo ratings yet
- துப்பறியும் சாம்பு - 3Document32 pagesதுப்பறியும் சாம்பு - 3Sathish RKNo ratings yet
- Understanding MACsec Security (MACsecDocument5 pagesUnderstanding MACsec Security (MACsecShivbraham Singh RajawatNo ratings yet
- SETTING UP GRE TUNNELSDocument4 pagesSETTING UP GRE TUNNELSamit_iihtdhn280No ratings yet
- IPSec Basics HandoutsDocument20 pagesIPSec Basics HandoutsJame JameNo ratings yet
- Cisco Aci Fundamentals 50xDocument320 pagesCisco Aci Fundamentals 50xvicofreNo ratings yet
- BBF EVPN Tutorial PDFDocument45 pagesBBF EVPN Tutorial PDFKishore TanukuNo ratings yet
- 6.-Policy Based Routing (PBR)Document11 pages6.-Policy Based Routing (PBR)jaiimeandres100% (1)
- Cisco VXLAN Configuration Lab Using Nexus 9000V DCNM & AnsibleDocument28 pagesCisco VXLAN Configuration Lab Using Nexus 9000V DCNM & AnsibleAlex MachadoNo ratings yet
- SD-Access NFR LabDocument29 pagesSD-Access NFR Labmihai pNo ratings yet
- Action Plan How To Crack CCIE RS V5Document12 pagesAction Plan How To Crack CCIE RS V5NguyễnThanhAnNo ratings yet
- Building Core Networks With OSPF, Is-Is, BGP, and MPLSDocument252 pagesBuilding Core Networks With OSPF, Is-Is, BGP, and MPLSWeiborao100% (1)
- Cisco Vxlan Config v1Document38 pagesCisco Vxlan Config v1DamisaNo ratings yet
- Private VLANsDocument4 pagesPrivate VLANsAlexShearNo ratings yet
- Extra Notes On IPsec VPNsDocument21 pagesExtra Notes On IPsec VPNsAlex MohNo ratings yet
- Squid Master Proxy ServerDocument8 pagesSquid Master Proxy ServerSiva RamNo ratings yet
- Cisco SD WAN Components - Detailed Explanation - IP With EaseDocument3 pagesCisco SD WAN Components - Detailed Explanation - IP With EasemvsnkraoNo ratings yet
- SOLIDserver Quickstart Hardware 2013Document2 pagesSOLIDserver Quickstart Hardware 2013proutNo ratings yet
- Ultimate Exam Preparation Kit 2015Document13 pagesUltimate Exam Preparation Kit 2015TimothyYeeNo ratings yet
- IPv6 and Packet TracerDocument98 pagesIPv6 and Packet Tracerobee1234No ratings yet
- Cisco Application Centric Infrastructure 4.1 With Vmware V1: About This DemonstrationDocument54 pagesCisco Application Centric Infrastructure 4.1 With Vmware V1: About This DemonstrationOscar Jiménez0% (1)
- EipPingSweeper v2.3 Setup GuideDocument13 pagesEipPingSweeper v2.3 Setup GuidedupontNo ratings yet
- BRKSPG 1000Document105 pagesBRKSPG 1000egriaNo ratings yet
- F5 Super-NetOps Program TrainingDocument251 pagesF5 Super-NetOps Program TrainingEng mtaherNo ratings yet
- Checkpoint R65 CLI Admin Guide PDFDocument17 pagesCheckpoint R65 CLI Admin Guide PDFHector Efrain Tovar IbarraNo ratings yet
- DO Ambassador20174Document142 pagesDO Ambassador20174TuPro FessionalNo ratings yet
- CCIE R&S Q and ADocument88 pagesCCIE R&S Q and Asujeet_hat100% (1)
- IPv6 Cisco LiveDocument115 pagesIPv6 Cisco LiveHuy NguyenNo ratings yet
- F5 Certification Prep Planning To SucceedDocument29 pagesF5 Certification Prep Planning To SucceedPadam Dhami100% (1)
- IPSec VPNs - An Overview - PresentationDocument157 pagesIPSec VPNs - An Overview - Presentationnamalka_omarNo ratings yet
- F5 Interview Questions and AnswersDocument13 pagesF5 Interview Questions and AnswersMahmoudAbdElGhaniNo ratings yet
- FoundationDocument55 pagesFoundationcisconotesNo ratings yet
- Pass4sure 400-101 CCIE R&S Written ExamDocument171 pagesPass4sure 400-101 CCIE R&S Written Examtestbells100% (1)
- JNCIE-SEC-11.a C7 NAT - PpsDocument37 pagesJNCIE-SEC-11.a C7 NAT - PpsYang JerryNo ratings yet
- Converged SDN Transport For CCIE SPv5 v202104Document326 pagesConverged SDN Transport For CCIE SPv5 v202104Joël FrançoisNo ratings yet
- Palo Alto Networks and AnsibleDocument4 pagesPalo Alto Networks and AnsibleJuan-PabloChaperoArenasNo ratings yet
- VXLAN Tutorial: THERDTOON TheerasasanaDocument36 pagesVXLAN Tutorial: THERDTOON TheerasasanaRaj KaranNo ratings yet
- Dna Licensing Switching Subscription BDMDocument60 pagesDna Licensing Switching Subscription BDMJames GrayNo ratings yet
- BPG Cisco ACIDocument38 pagesBPG Cisco ACIDavid Hernan Lira CarabantesNo ratings yet
- Chapter 10 Exam - CCNP Switch 2017Document10 pagesChapter 10 Exam - CCNP Switch 2017David Brincacequias100% (2)
- CCNP Switch Tema 10Document7 pagesCCNP Switch Tema 10Juan Pelaez0% (1)
- Cisco SD-Access TrainingDocument3 pagesCisco SD-Access TrainingAnonymous IS7QFvXNo ratings yet
- HSRP Vs VRRP Vs GLBPDocument2 pagesHSRP Vs VRRP Vs GLBPChristinah KenosiNo ratings yet
- EVPN GuideDocument1,965 pagesEVPN GuideDaniel Z.100% (1)
- Posture Cisco ISEDocument146 pagesPosture Cisco ISEhugobiarNo ratings yet
- BIG-IP Global Traffic Manager ImplementationsDocument153 pagesBIG-IP Global Traffic Manager ImplementationsjavirodzNo ratings yet
- Cisco Sdwan Design GuideDocument102 pagesCisco Sdwan Design GuideJohn TsigkrisNo ratings yet
- Alcatel-Lucent Multiprotocol Label Switching Student Guide v2-0 DLDocument672 pagesAlcatel-Lucent Multiprotocol Label Switching Student Guide v2-0 DLDiệp Lê HuyNo ratings yet
- JUNOS-to-Cisco IOS-XR Command Reference PDFDocument4 pagesJUNOS-to-Cisco IOS-XR Command Reference PDFasbandaraNo ratings yet
- BGP Next Hop SelfDocument9 pagesBGP Next Hop SelfNagendra SinghNo ratings yet
- F5 DNS Guide PDFDocument102 pagesF5 DNS Guide PDFRohanNo ratings yet
- Cisco DNA Center Appliance ConfigurationDocument14 pagesCisco DNA Center Appliance ConfigurationMiljan KostadinovićNo ratings yet
- Cisco Spiad - Labv1.3.1Document91 pagesCisco Spiad - Labv1.3.1fernando JmzNo ratings yet
- WiFi Troubleshooting CheatSheetDocument21 pagesWiFi Troubleshooting CheatSheetVee Pal100% (1)
- Conductive and Sensineural Hearing Loss & TinnitisDocument44 pagesConductive and Sensineural Hearing Loss & TinnitisJames StiltonNo ratings yet
- Pemicu 4: Indriani 405140178Document51 pagesPemicu 4: Indriani 405140178Ind MatthewNo ratings yet
- THEEARDocument9 pagesTHEEARapi-3822433No ratings yet
- Group 3 - BSN 2BDocument16 pagesGroup 3 - BSN 2BJan Clarisse RamosNo ratings yet
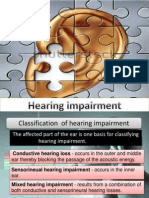
- Hearing Impairment Causes and TypesDocument27 pagesHearing Impairment Causes and TypesSteben MeuerteNo ratings yet
- Hearing ImpairmentDocument27 pagesHearing ImpairmentIrene Mendoza100% (1)
- Siegel's SpeculumDocument12 pagesSiegel's SpeculumDr Sravya M VNo ratings yet
- Viral ConjunctivitisDocument30 pagesViral ConjunctivitisDr Sravya M VNo ratings yet
- Anatomy of EyelidsDocument25 pagesAnatomy of EyelidsDr Sravya M VNo ratings yet
- TinnitusDocument18 pagesTinnitusDr Sravya M VNo ratings yet
- Kapala Rogas - ModernDocument23 pagesKapala Rogas - ModernDr Sravya M VNo ratings yet
- Physiology of HearingDocument30 pagesPhysiology of HearingDr Sravya M VNo ratings yet
- Examination of EyeDocument39 pagesExamination of EyeDr Sravya M VNo ratings yet
- Hearing EvaluationDocument151 pagesHearing EvaluationDr Sravya M VNo ratings yet
- Nursing Care Plan for Risk of Bleeding During PregnancyDocument4 pagesNursing Care Plan for Risk of Bleeding During PregnancybananakyuNo ratings yet
- Musculoskeletal Physiotherapy: Summary of ConditionsDocument22 pagesMusculoskeletal Physiotherapy: Summary of ConditionsJess MarriottNo ratings yet
- Dental Clinic Covid-19 FormsDocument4 pagesDental Clinic Covid-19 FormsButch EnalpeNo ratings yet
- Understanding Obstructive Sleep Apnea: Causes, Symptoms, and Treatment OptionsDocument27 pagesUnderstanding Obstructive Sleep Apnea: Causes, Symptoms, and Treatment OptionsdammieboiNo ratings yet
- HP Template PDFDocument2 pagesHP Template PDFnana100% (1)
- National Guideline On Integrated Vector Management 2020 NewDocument140 pagesNational Guideline On Integrated Vector Management 2020 NewNeha AmatyaNo ratings yet
- Pancytopenia Differential DiagnosisDocument40 pagesPancytopenia Differential DiagnosisFityan Aulia RahmanNo ratings yet
- Breach of Duty of CareDocument46 pagesBreach of Duty of CareJavier LimNo ratings yet
- FSRH Ukmec Summary September 2019Document11 pagesFSRH Ukmec Summary September 2019Kiran JayaprakashNo ratings yet
- Reasons BSN Students Are LateDocument4 pagesReasons BSN Students Are LateKizza SaavedraNo ratings yet
- Host and Environmental Factors Influencing Individual Human Cytokine Responses PDFDocument37 pagesHost and Environmental Factors Influencing Individual Human Cytokine Responses PDFLluis GomezNo ratings yet
- Clinical Considerations Case Catalog Screenshots and TimecodesDocument4 pagesClinical Considerations Case Catalog Screenshots and TimecodesnenitaNo ratings yet
- LPL - PSC Rajouri Garden Home Visit: Patientreportscsuperpanel - SP - General - Template01 - SC (Version: 7)Document2 pagesLPL - PSC Rajouri Garden Home Visit: Patientreportscsuperpanel - SP - General - Template01 - SC (Version: 7)Rabinder BakhshiNo ratings yet
- Rodela Et AlDocument14 pagesRodela Et AlDanish KhanNo ratings yet
- Tibb e NabviDocument15 pagesTibb e NabviAfraz Sheikh100% (2)
- ACHAI DLaboratory Actiivty 11 - The HeartDocument6 pagesACHAI DLaboratory Actiivty 11 - The HeartSYDNEY JILL ACHAINo ratings yet
- 3 Vs 6 Weeks IV Abx For OsteoDocument30 pages3 Vs 6 Weeks IV Abx For OsteoAmar AlkhafajiNo ratings yet
- Medical Terminology A Short Course 7th Edition Chabner Test BankDocument25 pagesMedical Terminology A Short Course 7th Edition Chabner Test BankKatherineMooretfqm100% (52)
- Basic First Aid NotesDocument9 pagesBasic First Aid NotesPaul SealyNo ratings yet
- Disease Prediction Using Machine Learning Algorithms2020 PDFDocument7 pagesDisease Prediction Using Machine Learning Algorithms2020 PDFSumati BaralNo ratings yet
- Gestational Diabetes Mellitus - : One Disease Two Lives at StakeDocument31 pagesGestational Diabetes Mellitus - : One Disease Two Lives at StakeSadia YousafNo ratings yet
- Combined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFDocument10 pagesCombined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFIsfan RialdyNo ratings yet
- Health6 q1 Mod2 Selfmanagement v1Document23 pagesHealth6 q1 Mod2 Selfmanagement v1BrianJessenMaweDignosNo ratings yet
- Recording Form 2 Masterlist of Grade 7 ROSEDocument2 pagesRecording Form 2 Masterlist of Grade 7 ROSEMELISSA MARTINNo ratings yet
- The Contributions of St. Cyprian: Perspectives On Epidemiology and Early ChristianityDocument15 pagesThe Contributions of St. Cyprian: Perspectives On Epidemiology and Early ChristianityLudimila Caliman CamposNo ratings yet
- Unit 2 General TestDocument5 pagesUnit 2 General TestAna Delia Rojas CañasNo ratings yet
- Daftar Pustaka: 2018, Badan Penelitian Dan Pengembangan Kesehatan, KementrianDocument9 pagesDaftar Pustaka: 2018, Badan Penelitian Dan Pengembangan Kesehatan, KementrianRan NisNo ratings yet
- Occupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesOccupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesMathea Cohen0% (1)
- Guide To Graphene Oxide DetoxDocument5 pagesGuide To Graphene Oxide Detoxeu100% (3)
- Module Goals: College of Criminal Justice EducationDocument8 pagesModule Goals: College of Criminal Justice EducationAila EchemaneNo ratings yet