You might also like
- Tracts of The Spinal CordDocument21 pagesTracts of The Spinal Corddr.a.k.gupta6924100% (10)
- Pathways For Neuroanatomy SCT: R. Heaslip M. JamesDocument15 pagesPathways For Neuroanatomy SCT: R. Heaslip M. Jameshzol83No ratings yet
- 3-Ascending Tracts of Spinal CordDocument28 pages3-Ascending Tracts of Spinal Cordmuhammad altaf100% (2)
- Neuroanatomy and Cerebrovascular CirculationDocument54 pagesNeuroanatomy and Cerebrovascular CirculationLemuel Pamaran del CastilloNo ratings yet
- Clinical Neurophysiology of The Vestibular System (001-057) PDFDocument57 pagesClinical Neurophysiology of The Vestibular System (001-057) PDFAriel CarterNo ratings yet
- Cerebellum: Principally Because Electrical Excitation of The CerebellumDocument42 pagesCerebellum: Principally Because Electrical Excitation of The Cerebellumdr_mksinhaNo ratings yet
- Brainstem (Yuni)Document34 pagesBrainstem (Yuni)Ayi Abdul Basith100% (2)
- Cns Anatomy & PhysiologyDocument25 pagesCns Anatomy & PhysiologyAgatha TerenciaNo ratings yet
- Excitable Cells: Monographs in Modern Biology for Upper School and University CoursesFrom EverandExcitable Cells: Monographs in Modern Biology for Upper School and University CoursesNo ratings yet
- CNS case proforma for stroke evaluationDocument2 pagesCNS case proforma for stroke evaluationRiyaSingh100% (1)
- Ascending TractsDocument42 pagesAscending TractsJustine Nyangaresi100% (2)
- Emergency Medicine EbookDocument642 pagesEmergency Medicine Ebookgulsoomro100% (1)
- Medical Facts and Mcq's Pediatric Surgery MCQDocument34 pagesMedical Facts and Mcq's Pediatric Surgery MCQMohammed Kassim Abdul Jabbar100% (3)
- Accommodation TestsDocument11 pagesAccommodation TestsNat Kang100% (1)
- Anatomy of BrainstemDocument66 pagesAnatomy of BrainstemFitria OctavianiNo ratings yet
- Pathology ChartsDocument21 pagesPathology Chartspadma maliniNo ratings yet
- Sa Dbmas Reboc Guide 2012Document34 pagesSa Dbmas Reboc Guide 2012Tony Abott100% (1)
- Anemia.: Seminar OnDocument24 pagesAnemia.: Seminar OnAlma Susan100% (1)
- Motor Functions of Spinal CordDocument43 pagesMotor Functions of Spinal CordEugeniu CoretchiNo ratings yet
- Ascending and Descending Spinal Tracts 2016Document20 pagesAscending and Descending Spinal Tracts 2016Ayodeji LuckyNo ratings yet
- Pyramidal SystemDocument52 pagesPyramidal SystemKowsalya SelvarajNo ratings yet
- Brain Stem: - Located BTWN The Cerebrum and The SCDocument41 pagesBrain Stem: - Located BTWN The Cerebrum and The SCnkuligowskiNo ratings yet
- Motoric Central Nervous System: Dr. Ridwan Harrianto MHSC (Om) SP - Ok, PakDocument47 pagesMotoric Central Nervous System: Dr. Ridwan Harrianto MHSC (Om) SP - Ok, PakMahasiswa StrugleNo ratings yet
- 4 Introduction to NeuroanatomyDocument76 pages4 Introduction to Neuroanatomyvbh8222No ratings yet
- 6 - Spinal CordDocument3 pages6 - Spinal CordasdfsNo ratings yet
- Assignment#4 Clinical Neuro Sciences: TOPIC: Describe Briefly The Clinical Testing of All Cranial NervesDocument3 pagesAssignment#4 Clinical Neuro Sciences: TOPIC: Describe Briefly The Clinical Testing of All Cranial NervesAlina ShaukatNo ratings yet
- Brain Stem, Limbic System and Others: By: SufitniDocument42 pagesBrain Stem, Limbic System and Others: By: Sufitniasa0411 behiraNo ratings yet
- 2.spinal CordDocument29 pages2.spinal CordPraneethaNo ratings yet
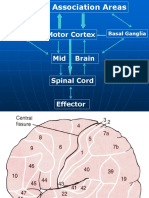
- Motor Cortex Mid Brain Spinal Cord Effector: Cerebellum Basal GangliaDocument19 pagesMotor Cortex Mid Brain Spinal Cord Effector: Cerebellum Basal GangliaMuhammad UmairNo ratings yet
- CEREBELUMDocument48 pagesCEREBELUMMarian GeorgeNo ratings yet
- Anat 6.5 Basal Ganglia - QuijanoDocument6 pagesAnat 6.5 Basal Ganglia - Quijanolovelots1234No ratings yet
- Brain Anatomy: Diencephalon, Brain Stem and Medulla SpinalisDocument36 pagesBrain Anatomy: Diencephalon, Brain Stem and Medulla SpinalisAngela FovinaNo ratings yet
- Physiology of Motor TractsDocument34 pagesPhysiology of Motor TractsNiko MartinNo ratings yet
- Midbrain - 2-18-07-2020Document26 pagesMidbrain - 2-18-07-2020Vinod SharmaNo ratings yet
- Spinal Cord: Navigation SearchDocument16 pagesSpinal Cord: Navigation SearchritzchoiNo ratings yet
- Motor Pathways Anatomy LecturesDocument24 pagesMotor Pathways Anatomy LecturesSindile MchunuNo ratings yet
- Localization in Clinical Neurology: Dr. Elsa GeorgeDocument64 pagesLocalization in Clinical Neurology: Dr. Elsa GeorgeElsa GeorgeNo ratings yet
- Descending Tracts: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeDocument39 pagesDescending Tracts: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmNo ratings yet
- The Spinal Cord: DR - SatyaDocument61 pagesThe Spinal Cord: DR - SatyacheckmateNo ratings yet
- PDF Document 6Document196 pagesPDF Document 6Erica Keil MoleNo ratings yet
- Anatomy of Spinal CordDocument39 pagesAnatomy of Spinal CordMai GaberNo ratings yet
- Sensory: Sensory (Ascending) Spinal TractsDocument24 pagesSensory: Sensory (Ascending) Spinal Tractsعبد الله الإمامNo ratings yet
- Central Nervous System 3rd Year Medicine Cerebellum & Basal GangliaDocument17 pagesCentral Nervous System 3rd Year Medicine Cerebellum & Basal GangliaGroup 14100% (1)
- L2 SBM Neuro - 2Document43 pagesL2 SBM Neuro - 2Sohil PatelNo ratings yet
- 2.motor Cotex and Tracts IDocument7 pages2.motor Cotex and Tracts Im6000000No ratings yet
- NS 5. Cerebrum SEPDocument28 pagesNS 5. Cerebrum SEPsanthiya rajendranNo ratings yet
- PBL 3 MDSC 2002 Upper or LowerDocument15 pagesPBL 3 MDSC 2002 Upper or LoweradaumedNo ratings yet
- The descending pathways that control motor activityDocument2 pagesThe descending pathways that control motor activityalmastar officeNo ratings yet
- Nro NotessafdaadDocument199 pagesNro NotessafdaadMunawwar AwaNo ratings yet
- Organization of Nervous System CNSDocument35 pagesOrganization of Nervous System CNSPayal MulaniNo ratings yet
- Cerebellum Structure and Connections GuideDocument97 pagesCerebellum Structure and Connections GuideAnonymous -No ratings yet
- Cerebellum and Basal Ganglia Anatomy and FunctionsDocument68 pagesCerebellum and Basal Ganglia Anatomy and FunctionsDivya AggarwalNo ratings yet
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 pagesSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriNo ratings yet
- Motor TractDocument4 pagesMotor TractRaden Achmad Candra PutraNo ratings yet
- Safari - Feb 21, 2024 at 12:17 PMDocument1 pageSafari - Feb 21, 2024 at 12:17 PMsyansyncNo ratings yet
- Spinal Cord Anatomy: Inha University Hospital Professor Yoon SHDocument34 pagesSpinal Cord Anatomy: Inha University Hospital Professor Yoon SHEstrella RomNo ratings yet
- Nervous Syste 1Document39 pagesNervous Syste 1Urwah KhanNo ratings yet
- Pyramidal and Extra Pyramidal Tract1Document23 pagesPyramidal and Extra Pyramidal Tract1agudabelieveNo ratings yet
- Physio. Psych Structure-Of-The-Nervous-System-Fact-SheetDocument7 pagesPhysio. Psych Structure-Of-The-Nervous-System-Fact-SheetJustynmae JusainNo ratings yet
- Tracts of Spinal Cord: Dr. Fathima TasneemDocument31 pagesTracts of Spinal Cord: Dr. Fathima TasneemMinaz PatelNo ratings yet
- The Midbrain and Important ConnectionsDocument118 pagesThe Midbrain and Important ConnectionsBaguma MichaelNo ratings yet
- Anatomi Dan Fisiologi Sistem PersyarafanDocument37 pagesAnatomi Dan Fisiologi Sistem PersyarafanAnonymous xfBKTQfNo ratings yet
- Cerebro CerebellumDocument23 pagesCerebro CerebellumJanani IyerNo ratings yet
- 2 NeuroanatomyDocument60 pages2 NeuroanatomyMeirina KhairatNo ratings yet
- p4 Extra Pyramidal SystemDocument19 pagesp4 Extra Pyramidal SystemHomeground entertainmentNo ratings yet
- Introduction To Brain: Prof. Ashraf HusainDocument58 pagesIntroduction To Brain: Prof. Ashraf Husainraanja2No ratings yet
- 21-Spinal Cord Tracts IDocument43 pages21-Spinal Cord Tracts ILeoNo ratings yet
- Spine LectureDocument55 pagesSpine LectureLeoNo ratings yet
- Lesson1 Intro Sensory SystemsDocument53 pagesLesson1 Intro Sensory SystemsLeoNo ratings yet
- Neuro 10 Cerebrovascular Supply StudentDocument36 pagesNeuro 10 Cerebrovascular Supply StudentLeoNo ratings yet
- (CC) Case Study 1 and 2Document11 pages(CC) Case Study 1 and 2Alyssa Nicole BarrettoNo ratings yet
- SRJI 3-4-2014 English Language Paperback Books in Acupuncture and Acupressure A 5-Year AnalysisDocument5 pagesSRJI 3-4-2014 English Language Paperback Books in Acupuncture and Acupressure A 5-Year AnalysisDr. Krishna N. SharmaNo ratings yet
- Veterinary Internal Medicine Handbook for Field CasesDocument88 pagesVeterinary Internal Medicine Handbook for Field CasesShakil MahmodNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Drug StudyDocument9 pagesDrug StudyKAROL MARIAE LUZ ERESNo ratings yet
- List of Comparatives and SuperlativeDocument7 pagesList of Comparatives and SuperlativeInga JurjuNo ratings yet
- Gen Path Case StudyDocument3 pagesGen Path Case Studydex7reme0% (1)
- Emergency Management of Anaphylactic Shock in Dental Practice - A ReviewDocument10 pagesEmergency Management of Anaphylactic Shock in Dental Practice - A ReviewKaram SarhanNo ratings yet
- Geriatric Fracture Case - Multiple Osteoporotic Fractures: Case-Based Interactive Lecture/moderated Interactive SessionDocument24 pagesGeriatric Fracture Case - Multiple Osteoporotic Fractures: Case-Based Interactive Lecture/moderated Interactive SessionBoby HarulprionoNo ratings yet
- Ineffectuve Breathign PatternDocument2 pagesIneffectuve Breathign PatternDiana Marie Magango FranciaNo ratings yet
- Passed Arab Board Exam 2014 with Recommended ReferencesDocument5 pagesPassed Arab Board Exam 2014 with Recommended ReferencesMuhammed AbdulmajeedNo ratings yet
- Tla1 Midterm BSC100Document3 pagesTla1 Midterm BSC100AXCEL V. ANTOQUENo ratings yet
- Health Assess - Chapter 23 Key TermsDocument3 pagesHealth Assess - Chapter 23 Key TermsAllison Doubek GibsonNo ratings yet
- BS Nursing Program OutcomesDocument20 pagesBS Nursing Program Outcomesۦۦ JamesNo ratings yet
- Papier EpilepsieDocument5 pagesPapier EpilepsieCelebre MualabaNo ratings yet
- Anemia of Chronic DiseaseDocument5 pagesAnemia of Chronic DiseaseGufront MustofaNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Diagnose of Submandibular Abscess PDFDocument13 pagesDiagnose of Submandibular Abscess PDFElvitrianaNo ratings yet
- Covid19-Drug StudyDocument7 pagesCovid19-Drug StudynicoleNo ratings yet
- Danger Signs in NewbornDocument22 pagesDanger Signs in NewbornAbhirup BoseNo ratings yet
- Ophthalmic Manifestation in Langerhans Cell Histio PDFDocument4 pagesOphthalmic Manifestation in Langerhans Cell Histio PDFAmi MisiciNo ratings yet
- ABG InterpretationDocument1 pageABG InterpretationHyakaNo ratings yet