You might also like
- Hazards of Local AnesthesiaDocument44 pagesHazards of Local AnesthesiaIyad Abou-RabiiNo ratings yet
- Local Anesthesia: Classification, Mechanism of Action, Complications and Recent AdvancementsDocument80 pagesLocal Anesthesia: Classification, Mechanism of Action, Complications and Recent AdvancementsRiya JainNo ratings yet
- Local Complications of LaDocument29 pagesLocal Complications of LaaakiNo ratings yet
- Anesthetic Complications: Leonardo, Perey, Zhong, ZhouDocument29 pagesAnesthetic Complications: Leonardo, Perey, Zhong, ZhouRenee PereyNo ratings yet
- AnesthesiaDocument4 pagesAnesthesiaLory Lyn50% (4)
- The SURGICAL Experience: AnesthesiaDocument43 pagesThe SURGICAL Experience: AnesthesiaAngela CamilleNo ratings yet
- Anestesi Pada Operasi Mata by PikalDocument60 pagesAnestesi Pada Operasi Mata by PikalSyahpikal SahanaNo ratings yet
- Epinephrine Drug StudyDocument7 pagesEpinephrine Drug StudyJhoy Iris SarangayaNo ratings yet
- Addis Ababa University School of Anesthesia Complication of Neuraxial Anesthesia and Their ManagmentDocument66 pagesAddis Ababa University School of Anesthesia Complication of Neuraxial Anesthesia and Their ManagmentagatakassaNo ratings yet
- Drugs ORDocument17 pagesDrugs ORCatherine ZamoraNo ratings yet
- Snake Bite, ShockDocument5 pagesSnake Bite, ShockVIPIN V NAIRNo ratings yet
- ORDocument7 pagesORMay EvelynNo ratings yet
- AnafilaksisDocument27 pagesAnafilaksisAhmad ZakiNo ratings yet
- Seizure DisordersDocument38 pagesSeizure DisordersLydia Lopz MsnrncdNo ratings yet
- Local/Regional/Spinal Anaesthesia: DefinitionDocument4 pagesLocal/Regional/Spinal Anaesthesia: DefinitionThistell ThistleNo ratings yet
- Complications of Local AnesthesiaDocument59 pagesComplications of Local AnesthesiaNishithaNo ratings yet
- RLE OR - Drug StudyDocument6 pagesRLE OR - Drug Studyelijahdale.guillergan-05No ratings yet
- Syok Anafilaksis 1Document4 pagesSyok Anafilaksis 1Mariatun Zahro NasutionNo ratings yet
- Local Anesthesia: Local and Systemic ComplicationsDocument6 pagesLocal Anesthesia: Local and Systemic ComplicationsBunga Erlita RosaliaNo ratings yet
- Anaphylactic ShockDocument25 pagesAnaphylactic ShockMaham BushraNo ratings yet
- Reaksi Anafilaksis - Dr. Prabowo WicaksonoDocument33 pagesReaksi Anafilaksis - Dr. Prabowo WicaksonoAnindya FloritaNo ratings yet
- Anesthesia:: Perioperative Nursing ImplicationsDocument32 pagesAnesthesia:: Perioperative Nursing ImplicationsjamesbungoNo ratings yet
- Management Trigeminal NeuralgiaDocument28 pagesManagement Trigeminal NeuralgiaApeksha JadhavNo ratings yet
- Anaphylaxis FKGDocument33 pagesAnaphylaxis FKGMega PuspitaNo ratings yet
- Spinal Anes Drug StudyDocument12 pagesSpinal Anes Drug StudyNicosia Mae FerrerNo ratings yet
- Snakebite: Dhruva Chaudhry, Inder Paul Singh, and Surcharita RayDocument6 pagesSnakebite: Dhruva Chaudhry, Inder Paul Singh, and Surcharita RayHandjar DaNo ratings yet
- Principles of Periodontal SurgryDocument106 pagesPrinciples of Periodontal SurgrynusreenNo ratings yet
- AnesthesiaDocument18 pagesAnesthesiaZakria Al-HadadNo ratings yet
- Scorpion StingDocument10 pagesScorpion StingSadr AkrmNo ratings yet
- Local Complications of The Local Anesthesia: by Assist. Lec. Abrar Nizar AlattarDocument92 pagesLocal Complications of The Local Anesthesia: by Assist. Lec. Abrar Nizar Alattarelle70503No ratings yet
- Dealing With Emergencies in PHCDocument46 pagesDealing With Emergencies in PHCEsra Aljaffer100% (1)
- Aaaaa AaaaaaaaaaaaaaaDocument48 pagesAaaaa AaaaaaaaaaaaaaaYaneth Angeles Benavente mamaniNo ratings yet
- AnaphylaxisDocument39 pagesAnaphylaxisLydia Novalista100% (1)
- Local Anesthesia Classification Contents of Cartridge + Functions Ianb TechniqueDocument26 pagesLocal Anesthesia Classification Contents of Cartridge + Functions Ianb TechniqueatikaNo ratings yet
- Anaphylaxis: By: O. Ahmadi, MD. Professor Assistant of Esfahan Medical School, Emergency Department of Al-Zahra HospitalDocument39 pagesAnaphylaxis: By: O. Ahmadi, MD. Professor Assistant of Esfahan Medical School, Emergency Department of Al-Zahra HospitalBudi SetyanugrahaNo ratings yet
- Complications of Local Anesthesia: DR Amna Muzaffar BDS, Fcps Assistant Professor, OmfsDocument74 pagesComplications of Local Anesthesia: DR Amna Muzaffar BDS, Fcps Assistant Professor, OmfsAbdul MananNo ratings yet
- Asma Pada AnakDocument24 pagesAsma Pada AnaksevyarvintaNo ratings yet
- Local Complications: Cause Management Prevention I. Attributed To The Solution Used Overdose/ToxicityDocument4 pagesLocal Complications: Cause Management Prevention I. Attributed To The Solution Used Overdose/Toxicityzuperzilch1676No ratings yet
- Cesarean SectionDocument31 pagesCesarean Sectionjovan teopizNo ratings yet
- Tetanus FinalDocument45 pagesTetanus FinalSamra AhmadNo ratings yet
- Cesarean Section & CSEA Anesthesia Nursing CareDocument32 pagesCesarean Section & CSEA Anesthesia Nursing Carejovan teopizNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- Drug Study LidocaineDocument15 pagesDrug Study LidocaineFrancym R. BatengaNo ratings yet
- Manage Adverse Drug Reactions in Dental PracticeDocument24 pagesManage Adverse Drug Reactions in Dental Practiceandreas kevinNo ratings yet
- Asthma-1Document79 pagesAsthma-1DanishMandiNo ratings yet
- Regional Anesthesia TechniquesDocument49 pagesRegional Anesthesia TechniqueskhanmoinNo ratings yet
- Organophosphate Poisoning GuidelineDocument5 pagesOrganophosphate Poisoning Guidelinelamoleverde9297No ratings yet
- Local Anesthesia in Dental and Nerve BlockDocument42 pagesLocal Anesthesia in Dental and Nerve BlockRahul SrivastavaNo ratings yet
- Anesthesia For Opthalmological SurgeriesDocument69 pagesAnesthesia For Opthalmological SurgeriesRajesh MunigialNo ratings yet
- Medical Emergencies in The Dental OfficeDocument23 pagesMedical Emergencies in The Dental Officeতৌহিদ তপুNo ratings yet
- Medical EmergenciesDocument40 pagesMedical EmergenciesMuhammad Azeem Khan100% (1)
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- Anaphylaxis TADocument54 pagesAnaphylaxis TAUriko ZoeNo ratings yet
- Anesthesia Review: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryDocument42 pagesAnesthesia Review: Vic V. Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryAnil vaddiNo ratings yet
- Basics of Anaesthesia in Surgery (Final).PDFDocument30 pagesBasics of Anaesthesia in Surgery (Final).PDFhhewadamiri143No ratings yet
- Epinephrine DrugStudy WWW Rnpedia ComDocument4 pagesEpinephrine DrugStudy WWW Rnpedia ComIrish LigayaNo ratings yet
- Gastrointestinal System: Antihistamine Half-Life: Onset: Peaks: DurationDocument3 pagesGastrointestinal System: Antihistamine Half-Life: Onset: Peaks: DurationsyerlyNo ratings yet
- Anaesthesia in Ophthalmology 001Document37 pagesAnaesthesia in Ophthalmology 001pranab2506No ratings yet
- 2 LaDocument233 pages2 LaSudeep DkNo ratings yet
- Maternity Newborn Diagnoses ICD-9 To ICD-10-CM Code TranslationDocument3 pagesMaternity Newborn Diagnoses ICD-9 To ICD-10-CM Code TranslationNathanael ReyesNo ratings yet
- Femur fracture assessment and treatment exam questionsDocument8 pagesFemur fracture assessment and treatment exam questionsKwabena Amankwa100% (2)
- Guide to Salivary Gland NeoplasmsDocument28 pagesGuide to Salivary Gland Neoplasmsrameshparajuli14100% (1)
- Health7 Q2 W4Document6 pagesHealth7 Q2 W4Joseph RemolaNo ratings yet
- Referral SourceDocument10 pagesReferral SourceHumberto FuentesNo ratings yet
- SLU Pathology CBL Cases for Gastrointestinal and Liver PathologyDocument6 pagesSLU Pathology CBL Cases for Gastrointestinal and Liver PathologyAaron O. CafeNo ratings yet
- A Case Presentation On MeningitisDocument29 pagesA Case Presentation On MeningitisNeeta0% (1)
- Disaster P1examDocument9 pagesDisaster P1examJushua Opsima RuizNo ratings yet
- 3rd Mid CaseDocument32 pages3rd Mid CaseHarshini MakkenaNo ratings yet
- Modified Bar Bending Method of Thoracoscopic NussDocument10 pagesModified Bar Bending Method of Thoracoscopic NussAlfadinAzzahrawaaniElNauvalNo ratings yet
- CKD With Uremic GastropathyDocument4 pagesCKD With Uremic GastropathyMaretha Laksmi MahananiNo ratings yet
- Citrus Black Spot PDFDocument2 pagesCitrus Black Spot PDFamuronegaduNo ratings yet
- MicroorganismsDocument12 pagesMicroorganismsMiggy GNo ratings yet
- After TURP: What to expectDocument2 pagesAfter TURP: What to expectvilla88No ratings yet
- Cwu 1 OrthoDocument14 pagesCwu 1 OrthoHakimah K. Suhaimi100% (1)
- Congenital Heart DiseasesDocument14 pagesCongenital Heart DiseasesEulane Ferrer100% (1)
- Bone Fracture Types, Causes, Signs and TreatmentDocument23 pagesBone Fracture Types, Causes, Signs and TreatmentGizachew AsimareNo ratings yet
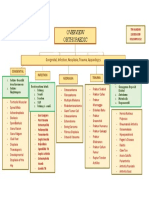
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Chapter 22 Streptococcus, Enterococcus and PneumococcusDocument73 pagesChapter 22 Streptococcus, Enterococcus and PneumococcusPriyanshiNo ratings yet
- Chart of Eye SymptomsDocument1 pageChart of Eye SymptomsRaghunandan RamanathanNo ratings yet
- Best Orthopedic Doctor in PatnaDocument4 pagesBest Orthopedic Doctor in PatnaOrtho PatnaNo ratings yet
- Pill CameraDocument21 pagesPill CameraAnil DsouzaNo ratings yet
- BarsDocument2 pagesBarsrichieerishiNo ratings yet
- Health Declaration Form D02Document1 pageHealth Declaration Form D02Hizwani ZainalNo ratings yet
- Esophageal Atresia: Elvita Rahmi DaulayDocument21 pagesEsophageal Atresia: Elvita Rahmi DaulayabdullahshiddiqadamNo ratings yet
- Food PoisoningDocument7 pagesFood PoisoningYoser ThamtonoNo ratings yet
- Causes and Types of Common Sports InjuriesDocument5 pagesCauses and Types of Common Sports InjuriesPedro HampaslupaNo ratings yet
- Bed Side Teaching Whipple'S Procedure: Submitted To-Sarita Nadiya Madam Submitted By-Ms - ManishaDocument8 pagesBed Side Teaching Whipple'S Procedure: Submitted To-Sarita Nadiya Madam Submitted By-Ms - ManishaManisha ShakyaNo ratings yet
- Updateoncanineparvoviral Enteritis: Elisa M. MazzaferroDocument19 pagesUpdateoncanineparvoviral Enteritis: Elisa M. MazzaferroAlfian Yusak MuzakiNo ratings yet
- By Jihad Anad EAU, Hinman Atlas, WebDocument43 pagesBy Jihad Anad EAU, Hinman Atlas, WebBayar A. AhmedNo ratings yet