You might also like
- Dental Procedures CodesDocument32 pagesDental Procedures CodesWil HectorNo ratings yet
- Antenatal Info Booklet Intuitive BirthDocument32 pagesAntenatal Info Booklet Intuitive Birthapi-223713414No ratings yet
- Ashton Manual English PDFDocument58 pagesAshton Manual English PDFMalissa Bowen100% (2)
- RSI For Nurses ICUDocument107 pagesRSI For Nurses ICUAshraf HusseinNo ratings yet
- Cataract And Small Pupil Management Manual Techniques: 2022, #1From EverandCataract And Small Pupil Management Manual Techniques: 2022, #1No ratings yet
- O&G OSCE by MaddyDocument287 pagesO&G OSCE by MaddyNariska Cooper100% (1)
- Test Bank For Medical Surgical Nursing 11th Edition Mariann M Harding Jeffrey Kwong Dottie Roberts Debra Hagler Courtney Reinisch DownloadDocument11 pagesTest Bank For Medical Surgical Nursing 11th Edition Mariann M Harding Jeffrey Kwong Dottie Roberts Debra Hagler Courtney Reinisch Downloadjenniferwilliamsonsoefnpykiz100% (23)
- Forceps Delivery and Vaccum ExtractionDocument113 pagesForceps Delivery and Vaccum Extractionchintu243435No ratings yet
- Hema I Chapter 3 - PhlebotomyDocument118 pagesHema I Chapter 3 - Phlebotomyderibew100% (1)
- Traveler's DiarrheaDocument17 pagesTraveler's DiarrheaAnonymous D29e00100% (1)
- Iv PrimingDocument16 pagesIv PrimingZahra jane A.No ratings yet
- Communication Skills For OSCEs Marking SchemeDocument26 pagesCommunication Skills For OSCEs Marking Schememarina shawky100% (1)
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- 5.forceps DeliveryDocument51 pages5.forceps Deliverysanthiyasandy100% (3)
- Difficult Airway ManagementDocument78 pagesDifficult Airway ManagementNedelcu Carmen100% (1)
- Vaccum DeliveryDocument24 pagesVaccum DeliveryBezawit TesfahunNo ratings yet
- Vacuum DeliveryDocument52 pagesVacuum Deliverynurul bahiyahNo ratings yet
- DR Rabiya Kaussar Tmo MCPS: Operative Vaginal DeliveryDocument45 pagesDR Rabiya Kaussar Tmo MCPS: Operative Vaginal DeliveryHaseeb AwanNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument33 pagesNew Microsoft Office PowerPoint PresentationVasuda Devi MalepatiNo ratings yet
- Ventouse CCDocument14 pagesVentouse CCNithiya NadesanNo ratings yet
- Assisted Vaginal Delivery Oct 2018Document27 pagesAssisted Vaginal Delivery Oct 2018Roberto MainaNo ratings yet
- Vacuum DeliveryDocument31 pagesVacuum DeliveryAparna LaxmanNo ratings yet
- Instrumental Delivery 2016Document44 pagesInstrumental Delivery 2016vrunda joshiNo ratings yet
- Forceps DeliveryDocument34 pagesForceps DeliveryBharat ThapaNo ratings yet
- Instrumental and Distructive DeliveryDocument66 pagesInstrumental and Distructive DeliveryDagnachew kasayeNo ratings yet
- Mod 2 2 ET UEDocument30 pagesMod 2 2 ET UEtsega tilahunNo ratings yet
- Assisted Vaginal DeliveryDocument26 pagesAssisted Vaginal Deliveryapi-3705046100% (5)
- The Incompetent Cervix 2Document30 pagesThe Incompetent Cervix 2api-3705046100% (3)
- Ekstraksi VakumDocument43 pagesEkstraksi VakumolipiaNo ratings yet
- Instrumental DeliveriesDocument108 pagesInstrumental DeliveriesAbunu TilayeNo ratings yet
- Lecture-31 Instrumental DeliveryDocument33 pagesLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaNo ratings yet
- Abnormal MaternityDocument280 pagesAbnormal Maternitymo7.v007No ratings yet
- Vitreous Prolapse ManagementDocument31 pagesVitreous Prolapse ManagementR.m. AndriyanNo ratings yet
- CH13 Assisted Vaginal BirthDocument39 pagesCH13 Assisted Vaginal BirthBrilliantine ChNo ratings yet
- Operative Vaginal Delivery: Ralphe Robert C. CajucomDocument41 pagesOperative Vaginal Delivery: Ralphe Robert C. CajucomThea ConcepcionNo ratings yet
- OBST OPERATIONS - SMHS LogoDocument47 pagesOBST OPERATIONS - SMHS LogoMax ZealNo ratings yet
- Vacuum ExtractionDocument28 pagesVacuum Extractionsirgute tamratNo ratings yet
- Ventouse Roll No 78Document17 pagesVentouse Roll No 78denanddon99No ratings yet
- Vacuum Extraction: Oleh: Putu Dion Pratama Puja 17710209Document17 pagesVacuum Extraction: Oleh: Putu Dion Pratama Puja 17710209Dion PratamaNo ratings yet
- Forcep Delivery: Dr. Niranjan ChavanDocument36 pagesForcep Delivery: Dr. Niranjan Chavandivine venturo100% (1)
- OB III Note - StudentsDocument13 pagesOB III Note - StudentsCheru DugaseNo ratings yet
- Assisted Vaginal Delivery Using The Vacuum ExtractorDocument7 pagesAssisted Vaginal Delivery Using The Vacuum ExtractorAhmad MuhyiNo ratings yet
- Management of HypospadiasDocument34 pagesManagement of HypospadiasAdebisiNo ratings yet
- Obstetric Forceps: Dr. Sourav Chowdhury Senior Resident OBG, IQCMCDocument22 pagesObstetric Forceps: Dr. Sourav Chowdhury Senior Resident OBG, IQCMCRitik AgarsenNo ratings yet
- Review On SPX CollectionDocument16 pagesReview On SPX CollectionkthmntsNo ratings yet
- Destructive OperationDocument12 pagesDestructive OperationBezawit TesfahunNo ratings yet
- MN Assistive Birth Methods RNDocument16 pagesMN Assistive Birth Methods RNBea HernandezNo ratings yet
- Cephalopelvic Disproportion, Obstructed Lab Our, UterineDocument49 pagesCephalopelvic Disproportion, Obstructed Lab Our, UterineKerod AbebeNo ratings yet
- OPERATIVE VAGINAL DELIVERY NewDocument95 pagesOPERATIVE VAGINAL DELIVERY NewBoruuf If GammachuuNo ratings yet
- RGU and MCU PPT Final For 18.9.23, BsmmuDocument46 pagesRGU and MCU PPT Final For 18.9.23, BsmmuMd.AlauddinNo ratings yet
- Obstetric Operations and Procedures - CompleteDocument46 pagesObstetric Operations and Procedures - CompleteMax ZealNo ratings yet
- Lumbar PunctureDocument25 pagesLumbar PunctureJacob BorongNo ratings yet
- UQUMed 5 PAP SmearDocument19 pagesUQUMed 5 PAP SmearAHMED .KNo ratings yet
- TOPIC 4 Specimen Collection & ProcessingDocument21 pagesTOPIC 4 Specimen Collection & ProcessingJhon Albert RobledoNo ratings yet
- Destructive Operation and Caesarian SectionDocument53 pagesDestructive Operation and Caesarian SectionVijith.V.kumar0% (1)
- Phlebotomy ComplicationsDocument11 pagesPhlebotomy ComplicationsGreniyelNo ratings yet
- ReservationDocument36 pagesReservationKyla Mae Fulache LevitaNo ratings yet
- Saline Lock: Health Emergency Medical Services Inc. (Wayne County Medical Control Authority)Document25 pagesSaline Lock: Health Emergency Medical Services Inc. (Wayne County Medical Control Authority)Priyanjali SainiNo ratings yet
- RPA Newborn Care Guidelines: Royal Prince Alfred Hospital Umbilical Venous CatheterisationDocument16 pagesRPA Newborn Care Guidelines: Royal Prince Alfred Hospital Umbilical Venous CatheterisationsalamredNo ratings yet
- Operative Vaginal Delivery (Ovd)Document35 pagesOperative Vaginal Delivery (Ovd)api-3705046No ratings yet
- IV Therapy PPT For StudentsDocument23 pagesIV Therapy PPT For StudentsMariefel Villanueva AlejagaNo ratings yet
- Obstetrics and GynecologyDocument44 pagesObstetrics and Gynecologyjaisanatandharma7No ratings yet
- Vacuum Extractor: Dr.K.J.JACOBDocument19 pagesVacuum Extractor: Dr.K.J.JACOBJacob KjNo ratings yet
- Pephalo Pelvicdisproportion &contracted PelvisDocument38 pagesPephalo Pelvicdisproportion &contracted PelvisAltynaiNo ratings yet
- Phlebotomy TechniquesDocument39 pagesPhlebotomy TechniquesnatalieshirleyNo ratings yet
- Cellulitis - Acute - NICE CKS PDFDocument40 pagesCellulitis - Acute - NICE CKS PDFDinu IuliaNo ratings yet
- Circulating Nurse in Divine Word Hospital, Tacloban CityDocument1 pageCirculating Nurse in Divine Word Hospital, Tacloban CityKenneth AbillarNo ratings yet
- Assessment Tool Clinical LabDocument1 pageAssessment Tool Clinical Labal gulNo ratings yet
- Womens Self-Management of AsthmaDocument24 pagesWomens Self-Management of AsthmaCenter for Managing Chronic DiseaseNo ratings yet
- Burn GuidelineDocument7 pagesBurn GuidelinegreenNo ratings yet
- Large CystDocument4 pagesLarge CystKin DacikinukNo ratings yet
- Challenges of Mass Casualty Management at A RegionDocument5 pagesChallenges of Mass Casualty Management at A RegionEbuwa AmadasunNo ratings yet
- Basics of Fetal MRIDocument80 pagesBasics of Fetal MRIjturos2003No ratings yet
- Healthy AgingDocument13 pagesHealthy AgingCarissa Mae Tapec EstradaNo ratings yet
- Herbalage Products KnowledgeDocument25 pagesHerbalage Products Knowledgemail9246No ratings yet
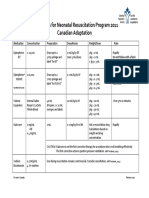
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Discharge InstructionDocument3 pagesDischarge Instructionolive oilNo ratings yet
- 2019 2020 Health History ExamDocument2 pages2019 2020 Health History Examsaranya purushothamanNo ratings yet
- What Causes CancerDocument2 pagesWhat Causes CancerSilla, KyshiaNo ratings yet
- Family Nursing Care Plan SeizuresDocument3 pagesFamily Nursing Care Plan SeizuresClaire AlcantaraNo ratings yet
- Prevalence of Behavioral and Emotional Disorders ADocument7 pagesPrevalence of Behavioral and Emotional Disorders AEricka GutiérrezNo ratings yet
- Reliable Diagnostic Center Pvt. LTD.: Mrs. Gopi DeviDocument1 pageReliable Diagnostic Center Pvt. LTD.: Mrs. Gopi DeviRahulJotwaniNo ratings yet
- Aninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017Document2 pagesAninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017pelangiNo ratings yet
- Arachnoid Cyst: From Wikipedia, The Free EncyclopediaDocument11 pagesArachnoid Cyst: From Wikipedia, The Free EncyclopediaOsama Bin RizwanNo ratings yet
- Perawatan Paliatif Pada Hiv/Aids: SolikinDocument45 pagesPerawatan Paliatif Pada Hiv/Aids: SolikinirpanNo ratings yet
- Modified Rhomboid Flap For Facial ReconstructionDocument3 pagesModified Rhomboid Flap For Facial ReconstructionahujasurajNo ratings yet
- ObjectiveDocument2 pagesObjectiveMarvinNo ratings yet
- Grover 2020Document2 pagesGrover 2020Riza Agung NugrahaNo ratings yet
- Antimicrobial Peptides From Scorpion Venoms PDFDocument23 pagesAntimicrobial Peptides From Scorpion Venoms PDFOrlando Pérez DelgadoNo ratings yet