You might also like
- Micro Cards MeningitisDocument6 pagesMicro Cards MeningitisFanny BudimanNo ratings yet
- Laboratory Diagnosis of Smallpox VirusDocument25 pagesLaboratory Diagnosis of Smallpox Virusማላያላም ማላያላምNo ratings yet
- CNS InfectionDocument10 pagesCNS InfectionShunqing ZhangNo ratings yet
- Neisseria MeningitidisDocument28 pagesNeisseria MeningitidisAshar AhmadNo ratings yet
- Lecture CSF 1Document7 pagesLecture CSF 1وسيم جمال مياسNo ratings yet
- Sumu PDFDocument30 pagesSumu PDFalokpalreshaNo ratings yet
- Meningitis (Completed)Document26 pagesMeningitis (Completed)seema83% (6)
- CNS InfectionsDocument3 pagesCNS InfectionsStefy BarranoNo ratings yet
- Neisse RiaDocument49 pagesNeisse RiaSubhada GosaviNo ratings yet
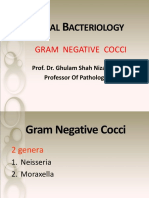
- L - 2 - GR (-) CocciDocument82 pagesL - 2 - GR (-) CocciFahim NadvyNo ratings yet
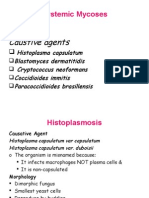
- Systemic MycosisDocument43 pagesSystemic MycosisAmirah AzamNo ratings yet
- Diagnostic VirologyDocument46 pagesDiagnostic VirologySarah DadoNo ratings yet
- Introduction To VirologyDocument30 pagesIntroduction To VirologyAkshaya MistryNo ratings yet
- Resistance Phenotypic of GramDocument25 pagesResistance Phenotypic of GramProiectulTauNo ratings yet
- Monocytogenes May Have Normal CSF WBC Results - Listeria May AlsoDocument4 pagesMonocytogenes May Have Normal CSF WBC Results - Listeria May AlsoAlfrien Ivanovich LarchsonNo ratings yet
- Bacterial Meningitis: - Maria Christma B. UmbañaDocument22 pagesBacterial Meningitis: - Maria Christma B. UmbañaMaria Christma UmbanaNo ratings yet
- Chapter II VirologyDocument116 pagesChapter II VirologyTofikNo ratings yet
- Neisseriaceae FamilyDocument15 pagesNeisseriaceae FamilyHamidreza RahmaniNo ratings yet
- Infecciones Del Sistema Nervioso CentralDocument14 pagesInfecciones Del Sistema Nervioso CentralJael ArgüellesNo ratings yet
- 1 PB PDFDocument6 pages1 PB PDFJayantiNo ratings yet
- Theme: Gramnegative Cocci (Gonococci, Meningococci)Document52 pagesTheme: Gramnegative Cocci (Gonococci, Meningococci)Mann SarwanNo ratings yet
- Clinical Virology (Dental)Document134 pagesClinical Virology (Dental)samar yousif mohamedNo ratings yet
- Neisseria & Moraxella: Done By: Tamara Khalel, Majd Shweiki, Aya SulimanDocument22 pagesNeisseria & Moraxella: Done By: Tamara Khalel, Majd Shweiki, Aya SulimanSalih TahsinNo ratings yet
- Microbiological Profiles of Neonatal Sepsis in Northern EgyptDocument12 pagesMicrobiological Profiles of Neonatal Sepsis in Northern EgyptAhmed AmerNo ratings yet
- Systemic Mycosis 06-07Document41 pagesSystemic Mycosis 06-07api-3699361No ratings yet
- Comparison of Culture and PCR Methods in The Diagnosis of Bacterial MeningitisDocument5 pagesComparison of Culture and PCR Methods in The Diagnosis of Bacterial Meningitisrais123No ratings yet
- 15medically Important Viruses PDFDocument75 pages15medically Important Viruses PDFdan ghaNo ratings yet
- Medically Important Viruses: The Methodical Manual For Medical StudentsDocument75 pagesMedically Important Viruses: The Methodical Manual For Medical Studentsdan ghaNo ratings yet
- Neisseria MeningitidisDocument53 pagesNeisseria MeningitidisPratibha AgarwalNo ratings yet
- VirologyDocument44 pagesVirologyREGGAN ROMARATENo ratings yet
- Gram Negative CocciDocument14 pagesGram Negative CocciRachel Marie M. GaniaNo ratings yet
- Cultivation of VirusDocument11 pagesCultivation of VirusSUTHAN50% (2)
- Mycology Revision Questions Dec 2020 2Document12 pagesMycology Revision Questions Dec 2020 2Jeshuah Jehopio100% (1)
- Diagnostic Laboratory Tests Epidemiology and Ecology: A. Specimens, Microscopic Examination, and CultureDocument3 pagesDiagnostic Laboratory Tests Epidemiology and Ecology: A. Specimens, Microscopic Examination, and CultureAnggaNo ratings yet
- Neonatal InfectionDocument56 pagesNeonatal InfectionAgust SalimNo ratings yet
- Bacterial Meningitis CaseDocument24 pagesBacterial Meningitis CaseALI MUMTAZNo ratings yet
- Laboratory Diagnosis of CMV Infection: A ReviewDocument6 pagesLaboratory Diagnosis of CMV Infection: A ReviewrendyjiwonoNo ratings yet
- CNS Infections 2013 - MKDocument54 pagesCNS Infections 2013 - MKmicroperadeniyaNo ratings yet
- CALDERON Bacteriology Worksheet With AnswersDocument3 pagesCALDERON Bacteriology Worksheet With AnswersJames Belgira TamayoNo ratings yet
- CNS Micro ImpulseDocument44 pagesCNS Micro Impulsedineshvd75No ratings yet
- LP After Correct.Document32 pagesLP After Correct.Academic Nurse. M.M AbbasNo ratings yet
- MICROBIOLOGY Pathogenic Gram-Positive Bacilli (Corynebacterium)Document7 pagesMICROBIOLOGY Pathogenic Gram-Positive Bacilli (Corynebacterium)Ravindra SinghNo ratings yet
- Diagnostic Approach To Chronic Meningitis (2018)Document19 pagesDiagnostic Approach To Chronic Meningitis (2018)CARZ 42No ratings yet
- Laboratory Diagnosis of Viral InfectionDocument35 pagesLaboratory Diagnosis of Viral InfectionHairul Anuar83% (18)
- Bacterio Practice QuestionsDocument25 pagesBacterio Practice QuestionsTorillo Kim100% (1)
- MoedhunduhnduhnDocument4 pagesMoedhunduhnduhnqkrvm59cgfNo ratings yet
- 3 Neonatal InfectionDocument56 pages3 Neonatal InfectiondindaamalaNo ratings yet
- CNS InfectionsDocument44 pagesCNS Infectionsfire_n_iceNo ratings yet
- New Chapter 3 Medical Microbiology (1) 2Document130 pagesNew Chapter 3 Medical Microbiology (1) 2Rani Faed SabraNo ratings yet
- 8.sti 2Document44 pages8.sti 2Mahrukh SiddiquiNo ratings yet
- Neonatal InfectionDocument56 pagesNeonatal InfectionGanesha Gamma 2017No ratings yet
- Am - Ve Cocci DPTDocument17 pagesAm - Ve Cocci DPTMaryam AsifNo ratings yet
- Davinci Medical AcademyDocument14 pagesDavinci Medical AcademyskNo ratings yet
- Microbial Diseases of The Nervous System: DR Sonnie P. Talavera 08162009 OlfuDocument162 pagesMicrobial Diseases of The Nervous System: DR Sonnie P. Talavera 08162009 Olfuone_nd_onlyu0% (1)
- Herpes Viruses 2Document36 pagesHerpes Viruses 2الطاهر زروقNo ratings yet
- MicroPara Report HandoutsDocument9 pagesMicroPara Report HandoutsKyla RamonesNo ratings yet
- Lecture - Gram Negative CocciDocument19 pagesLecture - Gram Negative CocciDina MahmoudNo ratings yet
- Staphylococcus Spp. FROM VARIOUS SAMPLESDocument15 pagesStaphylococcus Spp. FROM VARIOUS SAMPLESNuel EsguerraNo ratings yet
- New Microsoft Excel WorksheetDocument45 pagesNew Microsoft Excel WorksheetSanjay NadekarNo ratings yet
- BrainPOP Coronavirus QuizDocument1 pageBrainPOP Coronavirus QuizFlor GomezNo ratings yet
- Diseases of Passion FruitDocument18 pagesDiseases of Passion FruitRija Parfait RANDRIANANDRASANANo ratings yet
- IMMUNIZATIONDocument17 pagesIMMUNIZATIONZenasB.PalomaNo ratings yet
- ISO 6888-1:1999 + A1: 2003 StaphDocument5 pagesISO 6888-1:1999 + A1: 2003 StaphsylvanaNo ratings yet
- Case Studies in Infectious Disease: Books and MediaDocument2 pagesCase Studies in Infectious Disease: Books and MediaherrerachaimNo ratings yet
- Corona, False Alarm - PrefaceDocument5 pagesCorona, False Alarm - PrefaceChelsea Green PublishingNo ratings yet
- Introduction of Food Processing TechnologyDocument35 pagesIntroduction of Food Processing TechnologyFriz01No ratings yet
- Culture Staining Methods Microbiology LabDocument8 pagesCulture Staining Methods Microbiology LabJanessa AbastasNo ratings yet
- AMDAC-20211130-Slides-Merck (Updated With Backup)Document94 pagesAMDAC-20211130-Slides-Merck (Updated With Backup)Blue VelvetNo ratings yet
- Class 9 Biology Chapter 16 Diseases Causes and ControlDocument6 pagesClass 9 Biology Chapter 16 Diseases Causes and ControlwanroyNo ratings yet
- Arathi A.S:::: Patient Age / Sex 16 Y / Female BranchDocument1 pageArathi A.S:::: Patient Age / Sex 16 Y / Female BranchRick astley's microphoneNo ratings yet
- RAPID AST FROM BLOOD CULUTURE-Methodology - EUCAST - RAST - v1 - 20181126 PDFDocument3 pagesRAPID AST FROM BLOOD CULUTURE-Methodology - EUCAST - RAST - v1 - 20181126 PDFKhoa Vi Sinh BVCRNo ratings yet
- Report On HIV-AIDS WorkshopDocument3 pagesReport On HIV-AIDS WorkshopRaunak RoyNo ratings yet
- Sterilization: 25 % Cost Goes For Sterilization & Maintenance of Fermentation ProcessDocument59 pagesSterilization: 25 % Cost Goes For Sterilization & Maintenance of Fermentation ProcessAkshayaaRaveeNo ratings yet
- Vaccination 710428115244Document1 pageVaccination 710428115244arleesyaNo ratings yet
- EUA Assure Rapid2 Ifu PDFDocument3 pagesEUA Assure Rapid2 Ifu PDFArijit DebNo ratings yet
- NHMRC - Infection Control Guidelines-Accessible PDFDocument362 pagesNHMRC - Infection Control Guidelines-Accessible PDFMita Refanita100% (1)
- Kvir 13 2090071Document12 pagesKvir 13 2090071Familia PipekNo ratings yet
- Physical and Chemical Methods of SterilizationDocument27 pagesPhysical and Chemical Methods of SterilizationDanny Mel ManglaylayNo ratings yet
- Letter To Amazon Re: CoronavirusDocument2 pagesLetter To Amazon Re: CoronavirusSenator Cory Booker100% (4)
- Sanet - ST Handbook - Of.200.medicinal - Plants 2 PDFDocument2,076 pagesSanet - ST Handbook - Of.200.medicinal - Plants 2 PDFsmr76788% (8)
- Reference Books For CSIR-NET - BioTecNikaDocument11 pagesReference Books For CSIR-NET - BioTecNikaDr-Katari VenkateshNo ratings yet
- Mga Pamamaraan Upang Maiwasan Ang HIV at AIDS: (Alamin Ang Iyong ABC)Document4 pagesMga Pamamaraan Upang Maiwasan Ang HIV at AIDS: (Alamin Ang Iyong ABC)mhean azneitaNo ratings yet
- Lyphochek Assayed Chemistry Control Levels 1 and 2Document4 pagesLyphochek Assayed Chemistry Control Levels 1 and 2Gaurav MauryaNo ratings yet
- An Interactive Qualifying ProjectDocument130 pagesAn Interactive Qualifying ProjectjoyNo ratings yet
- Local Media2180871509351945489Document2 pagesLocal Media2180871509351945489Jenie Munar RosarioNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument14 pagesBest Practice & Research Clinical Obstetrics and GynaecologyIvonne CabreraNo ratings yet
- General Properties of VirusesDocument13 pagesGeneral Properties of VirusesMohammed Yousif mzoriNo ratings yet