You might also like
- 1.1 History Taking - SendDocument71 pages1.1 History Taking - Senddext9355No ratings yet
- 1.history TakingDocument60 pages1.history Takingdext9355No ratings yet
- History Taking and Physical ExaminationDocument53 pagesHistory Taking and Physical ExaminationBoruuf If GammachuuNo ratings yet
- History TakingDocument76 pagesHistory TakingyohanesNo ratings yet
- 2 - History Taking in PediatricsDocument59 pages2 - History Taking in Pediatricshawdeng xalitNo ratings yet
- HistoryDocument27 pagesHistoryabuhajerah15No ratings yet
- Pom MidtermsDocument692 pagesPom MidtermsGwyneth MendozaNo ratings yet
- Peds History (C FW06)Document35 pagesPeds History (C FW06)Prasad RauNo ratings yet
- Patient Examination: History: by Professor of Internal MedicineDocument47 pagesPatient Examination: History: by Professor of Internal MedicineMonqith YousifNo ratings yet
- History Taking: DR - Kamaran HassanDocument41 pagesHistory Taking: DR - Kamaran HassanSrush AliNo ratings yet
- 第一次课history-taking - 瞿立辉 2.29Document88 pages第一次课history-taking - 瞿立辉 2.29Mar ClrNo ratings yet
- Case History Form-1Document27 pagesCase History Form-1....No ratings yet
- ICM 01 History Taking (AOlajubelo-140611)Document39 pagesICM 01 History Taking (AOlajubelo-140611)AkbarNo ratings yet
- Adult Physical AssessmentDocument18 pagesAdult Physical AssessmentHa HahahahahaNo ratings yet
- Psychiatric History and Mental State Examination KabweDocument64 pagesPsychiatric History and Mental State Examination KabweFan Eli100% (4)
- Fnewfolder2historytakingicm 100519234626 Phpapp02Document32 pagesFnewfolder2historytakingicm 100519234626 Phpapp02cardiacanesthesiaNo ratings yet
- Anamnesia EnglishDocument33 pagesAnamnesia EnglishMalikNo ratings yet
- The Comprehensive Adult Health History Taking: For C-I StudentsDocument18 pagesThe Comprehensive Adult Health History Taking: For C-I StudentskderibNo ratings yet
- The Orthopedic History and Physical Exam GuideDocument28 pagesThe Orthopedic History and Physical Exam GuideAgriya Shresth100% (1)
- History TakingDocument2 pagesHistory TakingAmbar Rashid100% (1)
- Chapter One Introduction To Clinical MedicineDocument23 pagesChapter One Introduction To Clinical MedicinemulaewolloNo ratings yet
- History Taking2Document25 pagesHistory Taking2Capture UnseenNo ratings yet
- How to do a good case report write-upDocument34 pagesHow to do a good case report write-upNurhani MasjukiNo ratings yet
- Winnyfred Patience Ayugi Bsc. MidwiferyDocument30 pagesWinnyfred Patience Ayugi Bsc. MidwiferyAYO NELSONNo ratings yet
- Introduction To Internal Medicine - PPTMDocument30 pagesIntroduction To Internal Medicine - PPTMAddyNo ratings yet
- Patient Interviewing 440 2006Document20 pagesPatient Interviewing 440 2006Giovan GaulNo ratings yet
- 15.1. History Taking + ECG 1-肖培林Document125 pages15.1. History Taking + ECG 1-肖培林mirabel IvanaliNo ratings yet
- History Taking and Physical Examination, Level 5Document48 pagesHistory Taking and Physical Examination, Level 5CLEMENTNo ratings yet
- Paeds AssessmentDocument29 pagesPaeds AssessmentACERET, IVAN LAURENTINE G.No ratings yet
- 2023 Introduction To Physical DiagnosisDocument37 pages2023 Introduction To Physical DiagnosisNejibMohe Abagisa100% (1)
- Interviewing and The Health HistoryDocument18 pagesInterviewing and The Health HistoryWendz BouvierNo ratings yet
- Geriatric AssessmentDocument25 pagesGeriatric AssessmentGiovanni AnggastaNo ratings yet
- Mental Health Nursing: Psychiatric History CollectionDocument24 pagesMental Health Nursing: Psychiatric History Collectionbemina jaNo ratings yet
- Anamnesis Status GeneralisDocument103 pagesAnamnesis Status GeneralisHusnanMujiburrahmanNo ratings yet
- Internal First Partpdf 2Document178 pagesInternal First Partpdf 2Asma AhmedNo ratings yet
- Examination of the Head Neck 2018Document77 pagesExamination of the Head Neck 2018hayafalqasemiNo ratings yet
- MEDICAL HISTORY: A GUIDE TO TAKING A COMPLETE PATIENT HISTORYDocument19 pagesMEDICAL HISTORY: A GUIDE TO TAKING A COMPLETE PATIENT HISTORYPHARMACY 2021100% (1)
- Diseases of Choice: Diseases of Choice Prevention, Diseases of Choice Control and Diseases of Choice Health EducationFrom EverandDiseases of Choice: Diseases of Choice Prevention, Diseases of Choice Control and Diseases of Choice Health EducationNo ratings yet
- History Taking Guide - 70% Diagnosis from Patient HistoryDocument51 pagesHistory Taking Guide - 70% Diagnosis from Patient HistoryJAMES TONNY OKINYINo ratings yet
- History Taking - The Critical First Step in DiagnosisDocument51 pagesHistory Taking - The Critical First Step in DiagnosisJAMES TONNY OKINYINo ratings yet
- S1 - History Taking PresentationDocument37 pagesS1 - History Taking Presentationyouservezeropurpose113No ratings yet
- Imci Repaired NotesDocument136 pagesImci Repaired NotesGladys WarigheNo ratings yet
- W1-3 Iatric History and Physical Examination - LectureDocument124 pagesW1-3 Iatric History and Physical Examination - Lectureali fawziNo ratings yet
- HISTORYDocument28 pagesHISTORYrxmskdkd33No ratings yet
- Patient-Centered Medical History TakingDocument13 pagesPatient-Centered Medical History TakingAulia Azmi0% (1)
- Case History M.SCDocument10 pagesCase History M.SCRaksha RNNo ratings yet
- Patient InterviewDocument36 pagesPatient Interviewtomisin99gordonNo ratings yet
- Slide 1 - The History and Physical ExamDocument38 pagesSlide 1 - The History and Physical ExamCWT2010No ratings yet
- Health History Format Imad Lesson 1Document18 pagesHealth History Format Imad Lesson 1ellen_lomioNo ratings yet
- History Taking: DR Anwar H. SiddiquiDocument26 pagesHistory Taking: DR Anwar H. SiddiquiAssad mustafNo ratings yet
- Introduction HistoryDocument20 pagesIntroduction HistoryAyro Business CenterNo ratings yet
- Nursing History - A. Syanthiqah TirtaDocument3 pagesNursing History - A. Syanthiqah TirtaSanti TirtaNo ratings yet
- PT AssesmentDocument59 pagesPT AssesmentGetahun TsegayeNo ratings yet
- Assignment in PathoDocument8 pagesAssignment in PathoLyka Milo AvilaNo ratings yet
- History Taking For C-1Document48 pagesHistory Taking For C-1Merahit AberaNo ratings yet
- OSCE-Aid Presents: A Concise Guide to Taking a Thorough Patient HistoryDocument18 pagesOSCE-Aid Presents: A Concise Guide to Taking a Thorough Patient HistorycrystalsheNo ratings yet
- History Taking in Surgery: A Systematic ApproachDocument19 pagesHistory Taking in Surgery: A Systematic ApproachMohammad Farouq Omar100% (1)
- History TakingDocument28 pagesHistory TakingMutegeki AdolfNo ratings yet
- History Taking in Psychiatry-1Document30 pagesHistory Taking in Psychiatry-1Rajalingam JanarthanNo ratings yet
- Syndromic Management of STIsDocument1 pageSyndromic Management of STIsJoyNo ratings yet
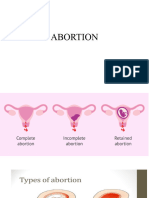
- ABORTIONDocument19 pagesABORTIONdanielndaa51No ratings yet
- 1.2.7 Abdominal Exam - SendDocument65 pages1.2.7 Abdominal Exam - Senddanielndaa51No ratings yet
- 1.2.5 Breast Examination - SendDocument48 pages1.2.5 Breast Examination - Senddanielndaa51100% (1)
- 1.2.1 Positions Used in Nursing - SendDocument45 pages1.2.1 Positions Used in Nursing - Sendlumbasi150No ratings yet
- Paediatric NeuroanaesthesiaDocument28 pagesPaediatric Neuroanaesthesiakoolstarone100% (1)
- Complications Bariatric SurgeryDocument8 pagesComplications Bariatric SurgeryThita Orrego100% (1)
- Drug Addiction: By: Ralph Berganio Abeygail Jimenez Maria Jasmine Maala Arleen Rose Roxas Margareth CortezDocument9 pagesDrug Addiction: By: Ralph Berganio Abeygail Jimenez Maria Jasmine Maala Arleen Rose Roxas Margareth CortezRikka TakanashiNo ratings yet
- FHC AaaaAAADocument5 pagesFHC AaaaAAAJUANJOSEFOXNo ratings yet
- Jin Gui Yao Lue PDFDocument64 pagesJin Gui Yao Lue PDFSergio Jesús Huapaya Gálvez75% (4)
- PD Reviewer For FinalsDocument5 pagesPD Reviewer For FinalsByrn YarteNo ratings yet
- Shëndeti Mendor I Fëmijlve Dhe Adoleshentëve Prizren Naim FanajDocument1 pageShëndeti Mendor I Fëmijlve Dhe Adoleshentëve Prizren Naim Fanajlulkuqe029No ratings yet
- CLL Case PresentationDocument17 pagesCLL Case PresentationAhmed EshraNo ratings yet
- Anatomy and Features of the NoseDocument29 pagesAnatomy and Features of the NoseMuhammad Waqar UlfatNo ratings yet
- Helping Physically Challenged ChildrenDocument2 pagesHelping Physically Challenged ChildrenSanthosh.S.UNo ratings yet
- 1 InfluenzaDocument7 pages1 InfluenzaElena MoldoveanuNo ratings yet
- Homotoxicology 6 Phase TableDocument1 pageHomotoxicology 6 Phase TableSamNo ratings yet
- 500 MG Tablet Analgesic - Antipyretic: UnilabDocument1 page500 MG Tablet Analgesic - Antipyretic: UnilabAngelie Nicole BordasNo ratings yet
- Ginger: A Versatile SpiceDocument10 pagesGinger: A Versatile SpiceAj Ceniza AmancioNo ratings yet
- Biology 9th Solving A Biological ProblemDocument5 pagesBiology 9th Solving A Biological Problemmhussainshigri786No ratings yet
- Face Masks Are Not Effective?Document5 pagesFace Masks Are Not Effective?Adam FernandezNo ratings yet
- Mood DisordersDocument108 pagesMood DisordersAngellene Firmalino50% (2)
- GAGAL GINJAL KRONIS DAN INDIKASI DIALISISDocument34 pagesGAGAL GINJAL KRONIS DAN INDIKASI DIALISISDjumadi AkbarNo ratings yet
- Module - I: 2.Milio'S Framework For PreventionDocument26 pagesModule - I: 2.Milio'S Framework For PreventionIanaCarandang100% (3)
- 01 - Introduction To MLGP PDFDocument29 pages01 - Introduction To MLGP PDFtinea nigraNo ratings yet
- Pharmacolgical Mangment of Diabetic Ketoacidosis: by Suliman OsmanDocument27 pagesPharmacolgical Mangment of Diabetic Ketoacidosis: by Suliman OsmanAymen OmerNo ratings yet
- Skor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermDocument9 pagesSkor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermMuhammad KhoiruddinNo ratings yet
- NCM 109 CMC at Risk PrelimDocument19 pagesNCM 109 CMC at Risk PrelimBeche May Lumantas100% (1)
- Knowledge, Attitudes and Practices of Hypertension Among Hypertensive Patients at Buchi Clinic, Kitwe, ZambiaDocument12 pagesKnowledge, Attitudes and Practices of Hypertension Among Hypertensive Patients at Buchi Clinic, Kitwe, ZambiaInternational Journal of Current Innovations in Advanced ResearchNo ratings yet
- Meningococcal InfectionsDocument1 pageMeningococcal Infectionsheng28369No ratings yet
- Neonatal Cholestasis GuideDocument28 pagesNeonatal Cholestasis GuideHafsaJabbarNo ratings yet
- IUFD Guide: Causes, Diagnosis and Management of Intrauterine Fetal DemiseDocument2 pagesIUFD Guide: Causes, Diagnosis and Management of Intrauterine Fetal Demisenurseon0% (1)
- Neurodevelopmental DisordersDocument5 pagesNeurodevelopmental DisordersKenth June GenobisNo ratings yet
- Brain Tumour GuideDocument11 pagesBrain Tumour GuidesonyNo ratings yet
- Brain Death AANDocument2 pagesBrain Death AANFabián Esteban Maturana Barra100% (1)