You might also like
- Peduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Document11 pagesPeduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Grace BrigondoNo ratings yet
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- 1100 Ultrasound of The Acute Abdomen 15 3Document84 pages1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016No ratings yet
- Askep PankreatitisDocument48 pagesAskep PankreatitisYeni DwiNo ratings yet
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoNo ratings yet
- Small & Large Bowel SlidesDocument17 pagesSmall & Large Bowel SlidesHunter ClontsNo ratings yet
- Pemicu 5Document75 pagesPemicu 5Cantika Monica LonanNo ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- Approach To A Patient With Upper GI BleedDocument42 pagesApproach To A Patient With Upper GI BleedMuhammad Naveed AslamNo ratings yet
- VolvulusDocument38 pagesVolvulusHector RaulNo ratings yet
- Management of Patients With Gastric and Duodenal DisordersDocument52 pagesManagement of Patients With Gastric and Duodenal DisordersTova LahaskyNo ratings yet
- Assessment and Management of Patients With Biliary DisordersDocument33 pagesAssessment and Management of Patients With Biliary DisorderssarahkaydNo ratings yet
- Disorders of PancreasDocument41 pagesDisorders of PancreasAbdullah BhattiNo ratings yet
- OncologicDocument187 pagesOncologicCherie BanzonNo ratings yet
- Dr.P.santhosh Kumar Post GraduateDocument22 pagesDr.P.santhosh Kumar Post GraduateSrilakshmi SathiyaNo ratings yet
- 01 - Signs and Symptoms of Git DisordersDocument51 pages01 - Signs and Symptoms of Git DisordersRere AnugrahNo ratings yet
- Acute GlumerulonephritisDocument77 pagesAcute GlumerulonephritisNicoleNo ratings yet
- Bowel ObstructionDocument36 pagesBowel ObstructionyoanNo ratings yet
- Urinary RetentionDocument28 pagesUrinary RetentionSchoeb MuhammadNo ratings yet
- Nephro Nursing - Urinary and Renal Dysfunctions (Part 2)Document53 pagesNephro Nursing - Urinary and Renal Dysfunctions (Part 2)ALLAINE MARIE TANNo ratings yet
- Intestinal Diseases in Cattle 2023Document30 pagesIntestinal Diseases in Cattle 2023Krystyna WędrychowskaNo ratings yet
- 4gastrointestinal DisorderDocument48 pages4gastrointestinal DisorderIzelwyn DaguioNo ratings yet
- Week3 PancreasDocument74 pagesWeek3 PancreasriverabeanicoNo ratings yet
- Alterations in Urinary FunctionDocument35 pagesAlterations in Urinary FunctionAaLona RobinsonNo ratings yet
- Colon 2Document56 pagesColon 2EnydLaRejNo ratings yet
- Patho SlidesDocument46 pagesPatho Slidesapi-400411160No ratings yet
- Approach To Abdominal Pain in EDDocument29 pagesApproach To Abdominal Pain in EDAneeq Nayer KhanNo ratings yet
- Chronic DiarrheaDocument38 pagesChronic DiarrheaShujina ZainabNo ratings yet
- 1) Ms II Hinkle PPT CH 49Document58 pages1) Ms II Hinkle PPT CH 49210411No ratings yet
- 1 Approach To DiarrheaDocument37 pages1 Approach To DiarrheamusabNo ratings yet
- CKD Case PresentationDocument25 pagesCKD Case PresentationMohamed Anwer NaleefNo ratings yet
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilNo ratings yet
- Acute AbdomenDocument53 pagesAcute AbdomenMahdi DiabNo ratings yet
- Biliary&Pancreas DisordersDocument34 pagesBiliary&Pancreas DisordersLarry De LaraNo ratings yet
- Assessment and Management of Patients With Biliary DisorderDocument50 pagesAssessment and Management of Patients With Biliary DisorderZanida ZainonNo ratings yet
- Gall StonesDocument26 pagesGall StonesNia SinghNo ratings yet
- CKD Case PresentationDocument25 pagesCKD Case PresentationMohamed Anwer NaleefNo ratings yet
- Askep HepaticDocument52 pagesAskep HepaticNia AnjarNo ratings yet
- Instestinal Obstruction UbthDocument34 pagesInstestinal Obstruction UbthDonald IDEDENo ratings yet
- CirrhosisDocument40 pagesCirrhosisyohannesNo ratings yet
- Etiology: 1.urinary RetentionDocument38 pagesEtiology: 1.urinary RetentionAbdurre YNo ratings yet
- Ulcerative ColitisDocument63 pagesUlcerative ColitismahalakshmiNo ratings yet
- By DR.: Haitham Mokhtar Mohamed Abd AllahDocument101 pagesBy DR.: Haitham Mokhtar Mohamed Abd AllahMohamed ElkadyNo ratings yet
- Colilithiasis 2Document53 pagesColilithiasis 2Worku KifleNo ratings yet
- Abdominal Distention and AscitesDocument49 pagesAbdominal Distention and AscitesNinaNo ratings yet
- Disorders of Biliary SystemDocument29 pagesDisorders of Biliary SystemAjibola OlamideNo ratings yet
- Renal MedsurgDocument14 pagesRenal MedsurgCliff Lois ╭∩╮⎷⎛⎝⎲⏝⏝⎲⎠⎷⎛╭∩╮ Ouano100% (1)
- Biliary Tract & Pancreas SlidesDocument17 pagesBiliary Tract & Pancreas SlidesHunter ClontsNo ratings yet
- Abdominal Emergencies Presentation (Recovered)Document126 pagesAbdominal Emergencies Presentation (Recovered)kityamuwesiNo ratings yet
- Abdominal Pain: LSU Medical Student Clerkship, New Orleans, LADocument48 pagesAbdominal Pain: LSU Medical Student Clerkship, New Orleans, LAAmd SolihinNo ratings yet
- Acute Chronic Kidney InjuryDocument29 pagesAcute Chronic Kidney InjuryPriya GKNo ratings yet
- 4.gall StoneDocument35 pages4.gall Stonejitendra magarNo ratings yet
- Gastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcDocument67 pagesGastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcMuath AlzghlellatNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388No ratings yet
- Abdominal Pain: Kerut SuardanaDocument48 pagesAbdominal Pain: Kerut SuardanaDiah SandiNo ratings yet
- Cholelithiasis When They Are in The Bile CholedocolithiasisDocument15 pagesCholelithiasis When They Are in The Bile Choledocolithiasishisabumohamed100% (1)
- Cellular AberrationDocument36 pagesCellular AberrationmidoNo ratings yet
- Acute AbdomenDocument29 pagesAcute AbdomenUmar AzlanNo ratings yet
- Hand HygeinDocument48 pagesHand Hygeinasma barhoomNo ratings yet
- Emergency DrugDocument264 pagesEmergency Drugasma barhoom100% (1)
- Arteriovenous MalformationDocument15 pagesArteriovenous Malformationasma barhoomNo ratings yet
- ABGs 2003Document3 pagesABGs 2003asma barhoomNo ratings yet
- Patel VentilatorAssociatedPneumoniaReductionDocument30 pagesPatel VentilatorAssociatedPneumoniaReductionasma barhoomNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Iap Guidelines On Rickettsial Diseases in ChildrenDocument7 pagesIap Guidelines On Rickettsial Diseases in Childrenitaa19No ratings yet
- Alice in Michigan: A Financial Hardship StudyDocument58 pagesAlice in Michigan: A Financial Hardship StudydaneNo ratings yet
- Approach To The Patient in Shock: by James Holencik, DODocument52 pagesApproach To The Patient in Shock: by James Holencik, DOLydia MamurNo ratings yet
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Tranumpreet Kaur 0064 Letter-Of-AcceptanceDocument3 pagesTranumpreet Kaur 0064 Letter-Of-AcceptanceTranum Kandiara (Tannu)No ratings yet
- Zika Virus and PregnancyDocument5 pagesZika Virus and PregnancyHerryNo ratings yet
- Good Practice Review - 8 - Revised2 PDFDocument323 pagesGood Practice Review - 8 - Revised2 PDFsteppevosNo ratings yet
- Lab # 5 Use Case and Activity Diagram: ObjectivesDocument7 pagesLab # 5 Use Case and Activity Diagram: ObjectivesmexiweNo ratings yet
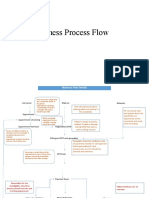
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- List of CosmeticsDocument9 pagesList of Cosmeticsasit_m0% (1)
- Allan ALH105 Week 3Document5 pagesAllan ALH105 Week 3alvin mwizNo ratings yet
- Jonsen 4 Box MethodDocument5 pagesJonsen 4 Box MethodsawsanNo ratings yet
- Global Poverty PowerPointDocument15 pagesGlobal Poverty PowerPointАдылхан БаймуратовNo ratings yet
- Internship PresentationDocument23 pagesInternship Presentationapi-556937362No ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- Grade 7 Health ModuleDocument22 pagesGrade 7 Health ModuleMeann Joy Barrios Mendoza100% (1)
- The Legal Bases of Special EducationDocument14 pagesThe Legal Bases of Special EducationMaria Dulcinea Basbas86% (7)
- Q - A Random 8Document5 pagesQ - A Random 8Yuuki Chitose (tai-kun)No ratings yet
- Wastemanagement 161028065024Document80 pagesWastemanagement 161028065024Atharva MansabdarNo ratings yet
- Cinnamon: Material Safety Data SheetDocument4 pagesCinnamon: Material Safety Data SheetJohn AnthraperNo ratings yet
- Developing Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersDocument6 pagesDeveloping Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersEugene GudimaNo ratings yet
- MSDS Cim PremixDocument3 pagesMSDS Cim PremixKiệt Lê TuấnNo ratings yet
- How May I Make My Penis More Robust? Answer That NowDocument2 pagesHow May I Make My Penis More Robust? Answer That NowEsbensen59TRUENo ratings yet
- Readers Digest Asia Feburary 2021Document134 pagesReaders Digest Asia Feburary 2021FURY FURIONNo ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Minimizing The Risk of Alzheimer S DiseaseDocument328 pagesMinimizing The Risk of Alzheimer S DiseaseLuis Raudales100% (1)
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)