You might also like
- Acute Myeloid LekumiaDocument34 pagesAcute Myeloid LekumiaBhuwan ThapaNo ratings yet
- Acute Myeloid Leukaemia (AML)Document27 pagesAcute Myeloid Leukaemia (AML)Immortal AndyNo ratings yet
- Acute Leukemia: Thirunavukkarasu MurugappanDocument22 pagesAcute Leukemia: Thirunavukkarasu MurugappanFelix Allen100% (1)
- Acute Myeloid LuekemiaDocument30 pagesAcute Myeloid LuekemiaKathleen DimacaliNo ratings yet
- Acute LeukemiaDocument25 pagesAcute LeukemiaТаня МарченкоNo ratings yet
- Pediatric Tumors 1Document35 pagesPediatric Tumors 1SarahNo ratings yet
- L-3 Introduction To LeukemiaDocument26 pagesL-3 Introduction To LeukemiaAbood dot netNo ratings yet
- Luekemia by Dr. WongelDocument63 pagesLuekemia by Dr. Wongelmogesie1995No ratings yet
- Acute Myeloblastic Leukemia AML: Dr. Amged H.AbdelrhmanDocument23 pagesAcute Myeloblastic Leukemia AML: Dr. Amged H.Abdelrhmanد. أمجد حسين عبد الرحمنNo ratings yet
- Acute Lymphoblastic Leukaemia (All) : DR Y. A Kawu Mbbs/Bds Lecture 4 DEC, 2023Document36 pagesAcute Lymphoblastic Leukaemia (All) : DR Y. A Kawu Mbbs/Bds Lecture 4 DEC, 2023Muhammad Modu BulamaNo ratings yet
- Acute Leukaemias Lecture-1Document39 pagesAcute Leukaemias Lecture-1MarvellousNo ratings yet
- Chronic Leukemia: Carlos Alfredo Cedeño RodríguezDocument24 pagesChronic Leukemia: Carlos Alfredo Cedeño RodríguezCarlos CedeñoNo ratings yet
- Acute Lymphoblastic Leukemia: Differential DiagnosisDocument6 pagesAcute Lymphoblastic Leukemia: Differential DiagnosisIma OhwNo ratings yet
- Pathology Lecture 2nd CourseDocument128 pagesPathology Lecture 2nd CourseAbdullah EssaNo ratings yet
- LeukemiaDocument48 pagesLeukemiaSandhya BasnetNo ratings yet
- PATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedDocument84 pagesPATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedAngelo HinonNo ratings yet
- Chronic Myeloid LeukaemiaDocument27 pagesChronic Myeloid Leukaemiaنواف الزهرانيNo ratings yet
- Acute LeukemiasDocument48 pagesAcute LeukemiaslaibaNo ratings yet
- Kuliah Kelainan Leukosit & RES - ZIADocument114 pagesKuliah Kelainan Leukosit & RES - ZIAannnisaNo ratings yet
- Chronic Myeloid LeukaemiaDocument30 pagesChronic Myeloid Leukaemiajismi vallachiraNo ratings yet
- Waldenstroms Macroglobulinemia (WM) FinalDocument57 pagesWaldenstroms Macroglobulinemia (WM) FinalnishNo ratings yet
- L14 Medicine Leukemia (Word)Document6 pagesL14 Medicine Leukemia (Word)Eslam Ibrahiem IbrahiemNo ratings yet
- Mielodisplasia, Neoplasia Maligna Hematopoyetica y Anemia AplasicaDocument24 pagesMielodisplasia, Neoplasia Maligna Hematopoyetica y Anemia AplasicakevinrdrixNo ratings yet
- Paediatric Acute Lymphoblastic LeukemiaDocument49 pagesPaediatric Acute Lymphoblastic LeukemiaKishoreChandraKoradaNo ratings yet
- Leukemia Lymphoma Skin Cancer - RubioDocument22 pagesLeukemia Lymphoma Skin Cancer - Rubiochristian pulmonesNo ratings yet
- Chronic Leukemia Lecture.Document47 pagesChronic Leukemia Lecture.sherifref3atNo ratings yet
- Myeloproliferative DisorderDocument36 pagesMyeloproliferative DisorderKalpana ShahNo ratings yet
- Acute Lymphocytic LeukemiaDocument7 pagesAcute Lymphocytic Leukemiamildred alidon100% (1)
- 01 Hemotological MalignaciesDocument92 pages01 Hemotological MalignaciesmarrymbigiNo ratings yet
- Medicine Seminar Combined-1Document30 pagesMedicine Seminar Combined-1Deepanshu KumarNo ratings yet
- Leukemias 2Document56 pagesLeukemias 2Y. Beatrice AbigailNo ratings yet
- Acute Leukemia: Dimas Bayu Tutik Harjianti A. FachruddinDocument41 pagesAcute Leukemia: Dimas Bayu Tutik Harjianti A. FachruddinFI 034 Mega Rahmawati MaulanaNo ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Patología de LeucocitosDocument25 pagesPatología de LeucocitosRicardo Castro MartínezNo ratings yet
- Hematologic Pathology p65-87Document23 pagesHematologic Pathology p65-87zeroun24100% (1)
- Leukemia Report Group 5Document56 pagesLeukemia Report Group 5Tiffany Luv AdriasNo ratings yet
- MDS and MPNDocument41 pagesMDS and MPNsamaNo ratings yet
- Hemopoietic SystemDocument28 pagesHemopoietic Systemyfzzhgv676No ratings yet
- Chronic Myeloid LeukaemiaDocument3 pagesChronic Myeloid LeukaemiaMayumie KumarageNo ratings yet
- Leukemia Pada AnakDocument33 pagesLeukemia Pada AnakandrianNo ratings yet
- WBC DisordersDocument45 pagesWBC DisordersyalahopaNo ratings yet
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]No ratings yet
- Cancer Nursing CareDocument36 pagesCancer Nursing CareSanvar Mal SoniNo ratings yet
- WBC Disorder PPT 2Document56 pagesWBC Disorder PPT 2YESHASWI PIKLENo ratings yet
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- Haematological Malignancies: Dr. Maruf Bin Habib Associate Professor of Medicine UamcDocument54 pagesHaematological Malignancies: Dr. Maruf Bin Habib Associate Professor of Medicine UamcSaifSeddikiNo ratings yet
- General Medicine Lec2 WBC DisordersDocument6 pagesGeneral Medicine Lec2 WBC DisordersAli MONo ratings yet
- All Aml NCCN 2023 HamidahDocument45 pagesAll Aml NCCN 2023 HamidahPPDS IPD ULMNo ratings yet
- Acute Leukemia15!11!2023جامعة دار السلامDocument42 pagesAcute Leukemia15!11!2023جامعة دار السلاماحمد احمدNo ratings yet
- TH LeukemiaDocument8 pagesTH Leukemiaأحمد علي حبيبNo ratings yet
- Leukimia Dan ThalasemiaDocument39 pagesLeukimia Dan ThalasemialeilaNo ratings yet
- Myeloproliferative Disorders (Bhs Inggris)Document57 pagesMyeloproliferative Disorders (Bhs Inggris)Denny DedenNo ratings yet
- Leukemia Myeloproliferation, Myelodysplasia: Lita Septina Peyakit Dalam FK UMSUDocument47 pagesLeukemia Myeloproliferation, Myelodysplasia: Lita Septina Peyakit Dalam FK UMSUJr SparkNo ratings yet
- Plasma Cell Disorders by DrAnjaliDocument59 pagesPlasma Cell Disorders by DrAnjaliMalavika MvNo ratings yet
- Leukemia 200331060831Document63 pagesLeukemia 200331060831Lolo TotoNo ratings yet
- Chronic Lymphoid LeukaemiaDocument23 pagesChronic Lymphoid LeukaemiaAyensuaNo ratings yet
- Leukaemia Lecture 01 - Aml - DRDocument69 pagesLeukaemia Lecture 01 - Aml - DRapi-273068056100% (1)
- Malignancy DR RashaDocument29 pagesMalignancy DR RashaRasha TelebNo ratings yet
- Mother Touch in Periodontal Therapy: Chorion MembraneDocument7 pagesMother Touch in Periodontal Therapy: Chorion MembraneInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gas Discharge VisualizationDocument8 pagesGas Discharge VisualizationNatt CabricsNo ratings yet
- The Implications of Vitamin D Status During Pregnancy On Mother and Her Developing ChildDocument11 pagesThe Implications of Vitamin D Status During Pregnancy On Mother and Her Developing ChildindahNo ratings yet
- Science-10 q4 Mod2 Biomolecules FinalCopy-1-2Document34 pagesScience-10 q4 Mod2 Biomolecules FinalCopy-1-2Christian Dar CabotajeNo ratings yet
- Experiment 2Document2 pagesExperiment 2kavikiran0% (1)
- 2nd SECOND QUARTER EXAM IN GRADE 7 SCIENCEDocument7 pages2nd SECOND QUARTER EXAM IN GRADE 7 SCIENCEJenny Rose Bingil89% (9)
- Elhers SyndromeDocument11 pagesElhers SyndromeFrancesca vitaleNo ratings yet
- From The Origin of Life To Evolutionary School of ThoughtDocument2 pagesFrom The Origin of Life To Evolutionary School of ThoughtJunell TadinaNo ratings yet
- Sir Altaf Hussain: Physiology Viva QuestionsDocument70 pagesSir Altaf Hussain: Physiology Viva QuestionsSamad LaghariNo ratings yet
- Unit 1 Workbook EvolutionDocument34 pagesUnit 1 Workbook EvolutionMarek BoothNo ratings yet
- Criminal Psychology Unit 1 Key TermsDocument3 pagesCriminal Psychology Unit 1 Key TermsSeanNo ratings yet
- M. Montesclaros Farms, Inc. Procedures Manual: Title Farrowing Stage (Selection Starts)Document3 pagesM. Montesclaros Farms, Inc. Procedures Manual: Title Farrowing Stage (Selection Starts)Beth TusoyNo ratings yet
- Ebook The Origins of Cellular Architecture Michael Lynch Online PDF All ChapterDocument69 pagesEbook The Origins of Cellular Architecture Michael Lynch Online PDF All Chapterelisa.leutwiler202100% (5)
- Aakash Rank Booster Test Series For NEET-2020Document17 pagesAakash Rank Booster Test Series For NEET-2020Anish TakshakNo ratings yet
- Two Year Medical (Phase-02) Test Planner - AY-2023-2024 Version 1.0 - TYM-EV-3,4,5-1Document2 pagesTwo Year Medical (Phase-02) Test Planner - AY-2023-2024 Version 1.0 - TYM-EV-3,4,5-1shreyansh keshariNo ratings yet
- Biology Igcse 0610 - m24 - QP - 12Document16 pagesBiology Igcse 0610 - m24 - QP - 12balooneypurpleNo ratings yet
- Mealey's Re Genetic Testing Motion in Holsten CaseDocument3 pagesMealey's Re Genetic Testing Motion in Holsten CaseKirk HartleyNo ratings yet
- Characteristics of Life UpdatedDocument12 pagesCharacteristics of Life UpdatedYla Mae Buo AcejoNo ratings yet
- Nicky Hayes & Sue Orell - Psychology, An IntroductionDocument508 pagesNicky Hayes & Sue Orell - Psychology, An IntroductionIordache OvidiuNo ratings yet
- Isaaa Brief 51 2015Document283 pagesIsaaa Brief 51 2015Julian Andres Tovar MedinaNo ratings yet
- 4TH Q Physical ScienceDocument14 pages4TH Q Physical Sciencemarvin agubanNo ratings yet
- Permanent TissuesDocument16 pagesPermanent TissuesRiyashika RNo ratings yet
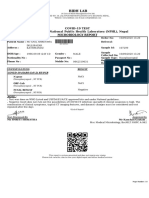
- Covid-19 Test Authorized by National Public Health Laboratory (NPHL), Nepal Microbiology ReportDocument1 pageCovid-19 Test Authorized by National Public Health Laboratory (NPHL), Nepal Microbiology ReportAnil ShresthaNo ratings yet
- HSSC BIOLOGY List of Practical and QuestionsDocument2 pagesHSSC BIOLOGY List of Practical and Questionsfareehasubhan123No ratings yet
- Clastic Cells in Orthodontic Treatment: Translational Challenges and Recent AdvancesDocument7 pagesClastic Cells in Orthodontic Treatment: Translational Challenges and Recent AdvancesDiego Andres Hincapie HerreraNo ratings yet
- CBSE Class 12 Biology Chapter 2 Sexual Reproduction in Flowering Plants Revision NotesDocument68 pagesCBSE Class 12 Biology Chapter 2 Sexual Reproduction in Flowering Plants Revision NotespranjaylakshitaNo ratings yet
- Restriction EnzymeDocument24 pagesRestriction EnzymeAlanGarciaNo ratings yet
- Chromosome Painting: Principles, Strategies and ScopeDocument178 pagesChromosome Painting: Principles, Strategies and ScopeBruna NatáliaNo ratings yet
- PGPR ScreeningDocument34 pagesPGPR ScreeningMaria BatoolNo ratings yet
- IB Exam Paper Gr. 11 HLDocument28 pagesIB Exam Paper Gr. 11 HLadambayNo ratings yet