You might also like
- Intrahepatic Pancreatic Pseudocyst Wayward Cyst 2024 International JournalDocument4 pagesIntrahepatic Pancreatic Pseudocyst Wayward Cyst 2024 International JournalRonald QuezadaNo ratings yet
- Complex Pattern of Colon Cancer Recurrence Including A Kidney Metastasis: A Case ReportDocument2 pagesComplex Pattern of Colon Cancer Recurrence Including A Kidney Metastasis: A Case Reportkangchih0331No ratings yet
- Acquired Colonic Atresia in A 4-Month Old Term Male Infant: A Rare Case ReportDocument3 pagesAcquired Colonic Atresia in A 4-Month Old Term Male Infant: A Rare Case ReportDenise CssNo ratings yet
- 11 Pyloric StenosisDocument4 pages11 Pyloric StenosiszapomannNo ratings yet
- Gastrointestinal Oncology: A Critical Multidisciplinary Team ApproachFrom EverandGastrointestinal Oncology: A Critical Multidisciplinary Team ApproachJanusz JankowskiNo ratings yet
- Complementary Roles of Interventional Radiology and Therapeutic Endoscopy in GastroenterologyDocument16 pagesComplementary Roles of Interventional Radiology and Therapeutic Endoscopy in GastroenterologyMANGNo ratings yet
- Poster Case Report Jecky Edited 2 (Final)Document1 pagePoster Case Report Jecky Edited 2 (Final)Johannes CordeNo ratings yet
- Annular PankreasDocument3 pagesAnnular PankreasAnonymous ocfZSRrrONo ratings yet
- Study On Surgical Management of Acute Intestinal Obstruction in AdultsDocument5 pagesStudy On Surgical Management of Acute Intestinal Obstruction in AdultsIzz “MOCHI” FadhliNo ratings yet
- Surgical Endoscopy Apr1998Document95 pagesSurgical Endoscopy Apr1998Saibo BoldsaikhanNo ratings yet
- Intussusception in AdultsDocument3 pagesIntussusception in AdultsKetan VagholkarNo ratings yet
- Naveed Et Al. - 2015 - Diagnosis and Management of An Esophagogastric Fistula As A Rare Complication of Nissen FundoplicationDocument2 pagesNaveed Et Al. - 2015 - Diagnosis and Management of An Esophagogastric Fistula As A Rare Complication of Nissen FundoplicationflashjetNo ratings yet
- Meredith 2010Document6 pagesMeredith 2010Ilma Kurnia SariNo ratings yet
- Europian Surgical Abstract 2 PDFDocument114 pagesEuropian Surgical Abstract 2 PDFDrAmmar MagdyNo ratings yet
- Intrauterine Device (IUD) in Bladder Stone: B Shetty, M VDocument3 pagesIntrauterine Device (IUD) in Bladder Stone: B Shetty, M VMangkubumi PutraNo ratings yet
- Another Caveat For Endoscopic Ultrasound– GuDocument1 pageAnother Caveat For Endoscopic Ultrasound– GuMsc Inf e prgjNo ratings yet
- Ewings Sarcoma - DescriptionDocument3 pagesEwings Sarcoma - DescriptionDamodara KumaranNo ratings yet
- Intestinal Duplication CystDocument2 pagesIntestinal Duplication Cystreeves_coolNo ratings yet
- 1.master Techniques in Surgery - Esophageal Surgery, 1E (2014)Document456 pages1.master Techniques in Surgery - Esophageal Surgery, 1E (2014)Raul Micu ChisNo ratings yet
- Appendectomy in BPJSDocument29 pagesAppendectomy in BPJSRinthoNo ratings yet
- Boerhaave Syndrome Case ReportDocument8 pagesBoerhaave Syndrome Case ReportDenisse SalazarNo ratings yet
- 2nd PeritonitisDocument11 pages2nd PeritonitisqweqweqwNo ratings yet
- 2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFDocument3 pages2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFNawzad SulayvaniNo ratings yet
- Pancreatitis NecroticaDocument7 pagesPancreatitis Necroticapancholin_9No ratings yet
- Wa0002Document14 pagesWa0002Katya RizqitaNo ratings yet
- 6665 PDFDocument4 pages6665 PDFerindah puspowatiNo ratings yet
- The Disappearing Abdominal Mass: Mesenteric Pseudocyst: Jasneet Singh Bhullar, MD, MS, Paraskevi Orfanou, MDDocument4 pagesThe Disappearing Abdominal Mass: Mesenteric Pseudocyst: Jasneet Singh Bhullar, MD, MS, Paraskevi Orfanou, MDDiyah SeptiRiyantiNo ratings yet
- Medicine: A Newborn Patient With Both Annular Pancreas and Meckel 'S DiverticulumDocument5 pagesMedicine: A Newborn Patient With Both Annular Pancreas and Meckel 'S DiverticulumAdrian UmbriaNo ratings yet
- JJ Intus Post RNY HJDocument29 pagesJJ Intus Post RNY HJRajesh MenonNo ratings yet
- Rectal Computer 1Document12 pagesRectal Computer 1Su-sake KonichiwaNo ratings yet
- AOCC IUS Primer Training Module Chapter 7Document14 pagesAOCC IUS Primer Training Module Chapter 7chengyucheung92No ratings yet
- Abdominal Wound ClosureDocument45 pagesAbdominal Wound ClosureKristabella GianinaNo ratings yet
- Dual Loop Reconstruction After Pancreaticoduodenectomy For A Previous Roux-En-Y Biliodigestive Anastomosis A Case ReportDocument2 pagesDual Loop Reconstruction After Pancreaticoduodenectomy For A Previous Roux-En-Y Biliodigestive Anastomosis A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Case Series of 5 Rare Abdominal EmergenciesDocument9 pagesA Case Series of 5 Rare Abdominal EmergenciesIJAR JOURNALNo ratings yet
- Bove 2012 Visc Mobiliz Adhesion RatDocument7 pagesBove 2012 Visc Mobiliz Adhesion RatQuiroprácticaParaTodosNo ratings yet
- How To Perform Gastrointestinal Ultrasound: Anatomy and Normal FindingsDocument12 pagesHow To Perform Gastrointestinal Ultrasound: Anatomy and Normal Findingsintan cNo ratings yet
- HHS Public Access: A Protocol For The Management of Adhesive Small Bowel ObstructionDocument15 pagesHHS Public Access: A Protocol For The Management of Adhesive Small Bowel ObstructionMuhammad Aziz FirdausNo ratings yet
- Retroperitoneal Appendicitis: A Surgical DilemmaDocument2 pagesRetroperitoneal Appendicitis: A Surgical DilemmaputraNo ratings yet
- Acalcolous PancreatitisDocument2 pagesAcalcolous PancreatitisalodiarkNo ratings yet
- The Surgical Management of Necrotizing Enterocolitis - July 2018Document4 pagesThe Surgical Management of Necrotizing Enterocolitis - July 2018Hengky TanNo ratings yet
- Combined Duodenal and Jejunal Atresia Forming A BiDocument3 pagesCombined Duodenal and Jejunal Atresia Forming A BiOvamelia JulioNo ratings yet
- HGMX 22 85 3 131-134Document4 pagesHGMX 22 85 3 131-134Julio BarajasNo ratings yet
- Aproximación Multidisciplinaria Al Diagnóstico y Tratamiento de La Obs Intestinal 2018Document124 pagesAproximación Multidisciplinaria Al Diagnóstico y Tratamiento de La Obs Intestinal 2018Jorge Nuñez LucicNo ratings yet
- 97438-Article Text-254324-1-10-20131121Document2 pages97438-Article Text-254324-1-10-20131121June Faith HacheroNo ratings yet
- 845 MazuskiDocument59 pages845 MazuskiZam HusNo ratings yet
- A 28-Year-Old Pregnant Woman With Endocervical CarcinomaDocument9 pagesA 28-Year-Old Pregnant Woman With Endocervical CarcinomaGerardo N. Pabón GallinoNo ratings yet
- Appendicitis: Oleh: Dr. Basaria ManurungDocument28 pagesAppendicitis: Oleh: Dr. Basaria ManurungBasaria 15No ratings yet
- Deep Infiltrating Endometriosis of The BDocument6 pagesDeep Infiltrating Endometriosis of The BСергей СадовниковNo ratings yet
- 1.2.2. Emergency Abdominal ImagingDocument51 pages1.2.2. Emergency Abdominal ImagingNoura AdzmiaNo ratings yet
- Rjy 033Document3 pagesRjy 033Natalindah Jokiem Woecandra T. D.No ratings yet
- Conclusions: Uodenal NjuriesDocument8 pagesConclusions: Uodenal NjuriesMargarita AucejoNo ratings yet
- Nihms 1796721Document17 pagesNihms 1796721CLINIC SURGERY 17THNo ratings yet
- Sister Mary Joseph Nodule As Cutaneous.9Document3 pagesSister Mary Joseph Nodule As Cutaneous.9Fernando MartinezNo ratings yet
- Treatment of Large Recurrent Aneurysmal Bone Cysts of Mandible: Transosseous Intralesional Embolization As An Adjunct To ResectionDocument6 pagesTreatment of Large Recurrent Aneurysmal Bone Cysts of Mandible: Transosseous Intralesional Embolization As An Adjunct To ResectionlalajanNo ratings yet
- A Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesDocument4 pagesA Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesSake Cinema21No ratings yet
- A Case Report: Dr. Nayef Al Abedallat Dr. Omar Suleiman Zarqa New Governmental HospitalDocument1 pageA Case Report: Dr. Nayef Al Abedallat Dr. Omar Suleiman Zarqa New Governmental HospitalOmar SuleimanNo ratings yet
- Ajcr 2010 1 2Document3 pagesAjcr 2010 1 2Muhammad Bilal MirzaNo ratings yet
- Gastric Perforation in Neonates: Analysis of Five Cases: Case ReportDocument3 pagesGastric Perforation in Neonates: Analysis of Five Cases: Case ReportwineniNo ratings yet
- Bove-Chapelle ViscMobilizAdhesionRatDocument7 pagesBove-Chapelle ViscMobilizAdhesionRatQuiroprácticaParaTodosNo ratings yet
- Tumor - Duodenal - 2022Document4 pagesTumor - Duodenal - 2022Berenice SanchezNo ratings yet
- EMT Past Papers 1122Document6 pagesEMT Past Papers 1122Ansar AliNo ratings yet
- 2ndyrAQUATICS AND SWIMMING MODULE 4Document18 pages2ndyrAQUATICS AND SWIMMING MODULE 4Zedy GullesNo ratings yet
- Examination of Cervical SpineDocument39 pagesExamination of Cervical SpinedrkanthikirangNo ratings yet
- Introduction To Human Anatomy and Physiology Lab FG 1011 1Document11 pagesIntroduction To Human Anatomy and Physiology Lab FG 1011 1CharmaineNo ratings yet
- Practical 1 - Skeletal AnatomyDocument11 pagesPractical 1 - Skeletal Anatomyjty4mkp59xNo ratings yet
- Scapula RetractionDocument2 pagesScapula RetractionQuốc HuyNo ratings yet
- Receiving and PositioningDocument45 pagesReceiving and PositioningCHALIE MEQUNo ratings yet
- Soal Ujian Neuroscience 2012 HJDDocument26 pagesSoal Ujian Neuroscience 2012 HJDCox AbeeNo ratings yet
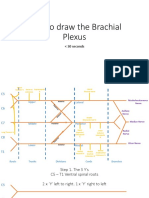
- How To Draw The Brachial PlexusDocument16 pagesHow To Draw The Brachial PlexusHNo ratings yet
- Snake BiteDocument66 pagesSnake BiteedfZSEADFsfsafafNo ratings yet
- Amputations: Amputations in The Workplace Safety TalkDocument3 pagesAmputations: Amputations in The Workplace Safety TalkIr Moise MatabaroNo ratings yet
- SNE-7100 - User ManualDocument35 pagesSNE-7100 - User ManualFirmawati Muslim SkepNo ratings yet
- Performance Checklist - ROMDocument3 pagesPerformance Checklist - ROMCrishaGarraNo ratings yet
- DSTC LDocument465 pagesDSTC LRizki Irwansyah100% (2)
- Shoulder Rehab Web Copy Aug15Document10 pagesShoulder Rehab Web Copy Aug15as asNo ratings yet
- Grit and Glory v5Document65 pagesGrit and Glory v5miguel ramos0% (1)
- Abbreviations and Symbols Commonly Used by Health Practitioners ActivitiesDocument10 pagesAbbreviations and Symbols Commonly Used by Health Practitioners ActivitiesAprilia PratiwiNo ratings yet
- Fractures of The Shafts of The Radius and Ulna in AdultDocument32 pagesFractures of The Shafts of The Radius and Ulna in AdultppdsNo ratings yet
- David Multi-Speciality Hospital.: No.277/1 Jamath Road, Opp To Vaniyambadi GH, Noorulahpet Vaniyambadi-635751Document2 pagesDavid Multi-Speciality Hospital.: No.277/1 Jamath Road, Opp To Vaniyambadi GH, Noorulahpet Vaniyambadi-635751SamJoe 14No ratings yet
- Task Risk Assessment Enter Company Name AMG: Risk Evaluation (Refer To Evaluation Form)Document3 pagesTask Risk Assessment Enter Company Name AMG: Risk Evaluation (Refer To Evaluation Form)Faizan ShabbirNo ratings yet
- 4 AxillaDocument31 pages4 AxillaRamesh KumarNo ratings yet
- Critical Essay Rough DraftDocument6 pagesCritical Essay Rough Draftapi-548821880No ratings yet
- Pe1Me: ReviewerDocument43 pagesPe1Me: ReviewerKylie BatitisNo ratings yet
- Science-6-LP-for-CSE - Skeletal SystemDocument11 pagesScience-6-LP-for-CSE - Skeletal SystemJECONIAH ADONANo ratings yet
- JLG-1930ES-2646ES-3246ES - EN Op. ManualDocument136 pagesJLG-1930ES-2646ES-3246ES - EN Op. Manualpakozdi.andorNo ratings yet
- Small Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)Document369 pagesSmall Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)ghimboasaNo ratings yet
- CHCDIS007 Empowering Disabled PeopleDocument22 pagesCHCDIS007 Empowering Disabled PeopleAshesh Basnet75% (8)
- OSHA 48, 30 by SPTIDocument117 pagesOSHA 48, 30 by SPTIGreen CaveNo ratings yet
- PCOME Ingram-Lopez Postmortem Examination ReportDocument8 pagesPCOME Ingram-Lopez Postmortem Examination ReportDylan SmithNo ratings yet
- Rusun Hemostatic Product Introduction 0625Document33 pagesRusun Hemostatic Product Introduction 0625Calvin hobbesNo ratings yet