You might also like
- Chest X Ray and CollapseDocument88 pagesChest X Ray and Collapseraseefa hamzaNo ratings yet
- Chest X-Ray InterpretationDocument116 pagesChest X-Ray Interpretation6130016019 AISYAH WANDA PUSPANINGTYASNo ratings yet
- Chest RadiographyDocument65 pagesChest RadiographyMunish Dogra100% (1)
- Pemeriksaan Foto Thorax Pada Anak-AnakDocument29 pagesPemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- RadioDocument58 pagesRadioMohSallakNo ratings yet
- Pemeriksaan Radiologi Pada Sistem Respirasi01Document115 pagesPemeriksaan Radiologi Pada Sistem Respirasi01Rendy NunuhituNo ratings yet
- Chest X-Ray Interpretation: Bucky Boaz, ARNP-CDocument101 pagesChest X-Ray Interpretation: Bucky Boaz, ARNP-CAnna DiaconuNo ratings yet
- Neonatal Chest X Ray 2019Document11 pagesNeonatal Chest X Ray 2019Ahmad ApriansahNo ratings yet
- Chest X-Ray InterpretationDocument104 pagesChest X-Ray InterpretationIbra Geeky100% (1)
- Neonatal Chest X-Ray-2019Document11 pagesNeonatal Chest X-Ray-2019madhu rathoreNo ratings yet
- Chest AssessmentDocument5 pagesChest Assessmentرحاب المريNo ratings yet
- Chest Xray BasicsDocument47 pagesChest Xray BasicsPartha GanesanNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayRizka RamadaniNo ratings yet
- Interpretasi Foto DadaDocument137 pagesInterpretasi Foto DadaRofi Irman100% (1)
- Radiography of The Thorax: BY Abubakar ADocument70 pagesRadiography of The Thorax: BY Abubakar AJameeluh TijjanyNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayMelissa Aina Mohd YusofNo ratings yet
- Chest X-Ray ReviewDocument145 pagesChest X-Ray ReviewHamid ShaalanNo ratings yet
- Respiratory System: Gemalyn BulawanDocument122 pagesRespiratory System: Gemalyn BulawanSofia Deneise AnasariasNo ratings yet
- X Thorax BeoordelenDocument135 pagesX Thorax BeoordelenmtescasuraNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayvmamikonNo ratings yet
- Chest Xray InterpretationDocument42 pagesChest Xray InterpretationLacey100% (3)
- Alterations in OxygenationDocument104 pagesAlterations in OxygenationMelchor Felipe Salvosa100% (1)
- (The Chest X-Ray)Document13 pages(The Chest X-Ray)RD Dha mhmdNo ratings yet
- Anatomy and Physiology of LungDocument29 pagesAnatomy and Physiology of LungKetheesaran Lingam100% (1)
- Introductio To:: SplanchnologyDocument36 pagesIntroductio To:: Splanchnologyrambabs369No ratings yet
- Adult Chest X-RayDocument60 pagesAdult Chest X-RayAnil DasNo ratings yet
- Chest X-Ray Interpretation A Structured Approach Radiology OSCEDocument1 pageChest X-Ray Interpretation A Structured Approach Radiology OSCEValentina SepúlvedaNo ratings yet
- RSDocument12 pagesRSKamalchandra NaikNo ratings yet
- Basic Chest RadDocument112 pagesBasic Chest Radtesfayegermame95.tgNo ratings yet
- Chest ImagingDocument51 pagesChest ImagingMikhayla ANo ratings yet
- Chest X-Ray Analysis 2023Document63 pagesChest X-Ray Analysis 2023CHARLOTTE DU PREEZNo ratings yet
- Anatomy, Physiology and Pathology of The RespiratoryDocument68 pagesAnatomy, Physiology and Pathology of The Respiratorytheresia_s_k100% (1)
- Radial Anatomy of The ThoraxDocument46 pagesRadial Anatomy of The ThoraxElijah KamaniNo ratings yet
- Interpretasi Dasar Foto Thoraks: Basuki Rachmat ICU Anak PJN HK JakartaDocument43 pagesInterpretasi Dasar Foto Thoraks: Basuki Rachmat ICU Anak PJN HK JakartaJanuary CoNiceNo ratings yet
- Chest Xray 2Document39 pagesChest Xray 2sushma shresthaNo ratings yet
- Pleura and LungsDocument7 pagesPleura and LungsNavisatul MutmainahNo ratings yet
- Pemeriksaan Fisik ParuDocument17 pagesPemeriksaan Fisik ParuMuhammad Luthfi AziziNo ratings yet
- Anatomy and Physiology of The Respiratory TractDocument49 pagesAnatomy and Physiology of The Respiratory TractshvnagaNo ratings yet
- Basic of Thorax Imaging - 10 September 2013 - by Robby HermawanDocument126 pagesBasic of Thorax Imaging - 10 September 2013 - by Robby HermawanenriNo ratings yet
- Diagnostic Imaging - 8 - Radiological Pathology - Lung Pathologies and Radiology in Specific Cases - Prof - Dr.i̇smet TAMERDocument35 pagesDiagnostic Imaging - 8 - Radiological Pathology - Lung Pathologies and Radiology in Specific Cases - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Chest X-Rays: Phillip Smith, BA, RRTDocument29 pagesChest X-Rays: Phillip Smith, BA, RRTAlexandra PopaNo ratings yet
- Chest X-Ray (CXR) Interpretation 2Document30 pagesChest X-Ray (CXR) Interpretation 2NaveedNo ratings yet
- Dr. Yash Kumar Achantani MBBS, MD (Radio-Diagnosis)Document24 pagesDr. Yash Kumar Achantani MBBS, MD (Radio-Diagnosis)Mayuri DhanushwarNo ratings yet
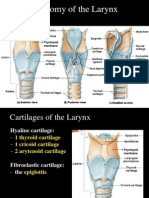
- Anatomy of The Larynx: Thyrohyoid MembraneDocument35 pagesAnatomy of The Larynx: Thyrohyoid MembraneVarsha Shende KhobragadeNo ratings yet
- Emergency UltrasoundDocument32 pagesEmergency UltrasoundChoga ArlandoNo ratings yet
- Respiratory AssessmentDocument25 pagesRespiratory AssessmentLIBIN PALLUPPETTAYIL JOSE100% (2)
- Physical Diagnoses: Respiratory SystemDocument72 pagesPhysical Diagnoses: Respiratory SystemAmanuel MaruNo ratings yet
- Mcqs RadiologyDocument65 pagesMcqs RadiologyAsmita BhattNo ratings yet
- Thoracic Imaging Radiographic BasicsDocument130 pagesThoracic Imaging Radiographic BasicsIsak ShatikaNo ratings yet
- Basic Interpretation of CXRDocument84 pagesBasic Interpretation of CXRHaluk AlibazogluNo ratings yet
- Clinical Therapeutics: Rhea Bernadette R. Danguilan Md-Iii BDocument20 pagesClinical Therapeutics: Rhea Bernadette R. Danguilan Md-Iii BMichelle Vera GabunNo ratings yet
- X Rays UG ClassDocument64 pagesX Rays UG ClassSwayam AroraNo ratings yet
- BronchiectasisDocument71 pagesBronchiectasisvijay1234568883No ratings yet
- Thorax LungsDocument128 pagesThorax LungsVernon MasakayanNo ratings yet
- CHEST X-RAY Presentation CVSDocument45 pagesCHEST X-RAY Presentation CVSNorsafrini Rita Ahmad100% (1)
- Medical Imaging - RadiologyDocument88 pagesMedical Imaging - RadiologyLe RobertNo ratings yet
- NucMed 1Document13 pagesNucMed 1John Paul MarasiganNo ratings yet
- Radthera 3Document23 pagesRadthera 3John Paul MarasiganNo ratings yet
- Lesson 1 Teaching StrategyDocument1 pageLesson 1 Teaching StrategyJohn Paul MarasiganNo ratings yet
- Spect CTDocument41 pagesSpect CTJohn Paul MarasiganNo ratings yet
- Cardiology - Echo Fate Card-2Document4 pagesCardiology - Echo Fate Card-2Mateen Shukri100% (2)
- EstudioDocument30 pagesEstudioSonia QuicenoNo ratings yet
- Perloff TOFDocument28 pagesPerloff TOFvamshidhNo ratings yet
- Theme 16-1 Chest TraumaDocument2 pagesTheme 16-1 Chest TraumaTaranbir Saini100% (3)
- Assessing The Thorax and The LungsDocument9 pagesAssessing The Thorax and The LungsChrizzia Del RosarioNo ratings yet
- Chest TrauDocument9 pagesChest TrauKaye CorNo ratings yet
- Revista Romana de Cardiologie - 2004Document49 pagesRevista Romana de Cardiologie - 2004LoredanaMunteanuNo ratings yet
- Lead GenerationDocument9 pagesLead GenerationMuddaserNo ratings yet
- How To Read A Chest X-RayDocument3 pagesHow To Read A Chest X-RayKristina KostadinovskaNo ratings yet
- Report Tetralogy of FallotDocument3 pagesReport Tetralogy of FallotLieana AguilarNo ratings yet
- Grade 1 Pattern of LV Diastolic FillingDocument3 pagesGrade 1 Pattern of LV Diastolic FillingNicoleNo ratings yet
- Study Guide For Lecture Exam 3. Heart.: Pulmonary CirculationDocument4 pagesStudy Guide For Lecture Exam 3. Heart.: Pulmonary CirculationmakNo ratings yet
- Schedule D: Drug Regulatory Authority of PakistanDocument4 pagesSchedule D: Drug Regulatory Authority of Pakistanمحمد عبداللہ چوہدریNo ratings yet
- Standardized Echo Report Rev1Document38 pagesStandardized Echo Report Rev1dgina8800100% (1)
- HFAI ProgrammeDocument40 pagesHFAI ProgrammejayjayshrigokuleshNo ratings yet
- Anatomi Kardiovaskular 4Document10 pagesAnatomi Kardiovaskular 4Lie LhianzaNo ratings yet
- CVS and RSDocument132 pagesCVS and RSclareawambuiNo ratings yet
- Exercise 1: Label and Explain The Blood CirculationDocument2 pagesExercise 1: Label and Explain The Blood CirculationKiana Ramosa100% (1)
- Congenital Heart Disease (CHD) : Lecture For C-I StudentsDocument89 pagesCongenital Heart Disease (CHD) : Lecture For C-I StudentsGomathi ShankarNo ratings yet
- ? - Pedia MidtermsDocument18 pages? - Pedia Midtermsysabel.mendozaNo ratings yet
- PANCE Prep Pearls Valvular Disease PDFDocument4 pagesPANCE Prep Pearls Valvular Disease PDFkatNo ratings yet
- 4 2 3 A Ekg Student Response Sheet (Revised 2 23 15)Document8 pages4 2 3 A Ekg Student Response Sheet (Revised 2 23 15)api-281824634100% (1)
- CABG PCS CodingDocument3 pagesCABG PCS CodingVikas MaheshwariNo ratings yet
- Murmurs Made Easy PDFDocument3 pagesMurmurs Made Easy PDFTanya GnNo ratings yet
- Nomograms of Fetal Cardiac Dimensions at 18-41 Weeks of GestationDocument12 pagesNomograms of Fetal Cardiac Dimensions at 18-41 Weeks of GestationMarco Julcamoro AsencioNo ratings yet
- Acute Respiratory Distress Syndrome: By: Ben Meron MichalDocument13 pagesAcute Respiratory Distress Syndrome: By: Ben Meron Michalmichal ben meronNo ratings yet
- Oxford University Press - Online Resource Centre - Multiple Choice QuestionsDocument4 pagesOxford University Press - Online Resource Centre - Multiple Choice QuestionsJublant JimmiyahNo ratings yet
- Pleural PathologiesDocument34 pagesPleural PathologiesAshwani RamawatNo ratings yet
- Basic ECG For BeginnersDocument109 pagesBasic ECG For BeginnersEmad ElhusseinNo ratings yet
- Respiratory Case Study 6 PDFDocument2 pagesRespiratory Case Study 6 PDFZainab HakeemNo ratings yet