You might also like
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- The Ultimate OCN Exam Practice Questions and Exam Prep Toolkit: A Comprehensive OCN Study Guide with 800 Practice Questions and AnswersFrom EverandThe Ultimate OCN Exam Practice Questions and Exam Prep Toolkit: A Comprehensive OCN Study Guide with 800 Practice Questions and AnswersNo ratings yet
- NCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsFrom EverandNCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsNo ratings yet
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationFrom EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationNo ratings yet
- Ambulatory Care Coordinator - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandAmbulatory Care Coordinator - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Hospitalist Recruitment and Retention: Building a Hospital Medicine ProgramFrom EverandHospitalist Recruitment and Retention: Building a Hospital Medicine ProgramNo ratings yet
- Ccrn Certification Examination Practice Questions and Answers with Rationale: First EditionFrom EverandCcrn Certification Examination Practice Questions and Answers with Rationale: First EditionRating: 5 out of 5 stars5/5 (1)
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- Medical Utilization Review Coordinator - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandMedical Utilization Review Coordinator - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- A Handbook for Student Nurses, 2015–16 edition: Introducing Key Issues Relevant to PracticeFrom EverandA Handbook for Student Nurses, 2015–16 edition: Introducing Key Issues Relevant to PracticeRating: 5 out of 5 stars5/5 (2)
- Crunch Time Review for the Certified Nursing Assistant (CNA) ExamFrom EverandCrunch Time Review for the Certified Nursing Assistant (CNA) ExamNo ratings yet
- Textbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationFrom EverandTextbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationNo ratings yet
- Evaluation of a Dialogical Psychologically Informed Environment (PIE) Pilot: Addressing homelessness, re-offending, substance abuse, and mental illnessFrom EverandEvaluation of a Dialogical Psychologically Informed Environment (PIE) Pilot: Addressing homelessness, re-offending, substance abuse, and mental illnessNo ratings yet
- Clinical Documentation Specialist - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandClinical Documentation Specialist - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Health & Quality - through customers experiencesFrom EverandHealth & Quality - through customers experiencesRating: 5 out of 5 stars5/5 (1)
- Comprehensive Care Coordination for Chronically Ill AdultsFrom EverandComprehensive Care Coordination for Chronically Ill AdultsCheryl SchraederNo ratings yet
- The Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayFrom EverandThe Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayNo ratings yet
- Nursing Informatics: Scope and Standards of PracticeFrom EverandNursing Informatics: Scope and Standards of PracticeRating: 4 out of 5 stars4/5 (6)
- Clinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandClinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Therapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyFrom EverandTherapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyNo ratings yet
- Quality and Safety in Nursing: A Competency Approach to Improving OutcomesFrom EverandQuality and Safety in Nursing: A Competency Approach to Improving OutcomesGwen SherwoodNo ratings yet
- Cancer Registry Manager - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandCancer Registry Manager - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- A Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeFrom EverandA Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeNo ratings yet
- Multiple Choice Questions in Healthcare QualityFrom EverandMultiple Choice Questions in Healthcare QualityRating: 4 out of 5 stars4/5 (8)
- Nursing Administration: Scope and Standards of PracticeFrom EverandNursing Administration: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (3)
- Textbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionFrom EverandTextbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionNo ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Laboratory Assessment of Nutritional Status: Bridging Theory & PracticeFrom EverandLaboratory Assessment of Nutritional Status: Bridging Theory & PracticeRating: 1 out of 5 stars1/5 (1)
- Next Generation NCLEX-RN Prep 2023-2024: Practice Test + Proven StrategiesFrom EverandNext Generation NCLEX-RN Prep 2023-2024: Practice Test + Proven StrategiesRating: 5 out of 5 stars5/5 (1)
- Next Generation NCLEX-PN Prep 2023-2024: Practice Test + Proven StrategiesFrom EverandNext Generation NCLEX-PN Prep 2023-2024: Practice Test + Proven StrategiesNo ratings yet
- Assessing Universal Health Coverage for Breast Cancer Management: Is the Service and Financial Coverage Adequate for Preventive and Curative Care?From EverandAssessing Universal Health Coverage for Breast Cancer Management: Is the Service and Financial Coverage Adequate for Preventive and Curative Care?No ratings yet
- Correctional Nursing: Scope and Standards of Practice, Third EditionFrom EverandCorrectional Nursing: Scope and Standards of Practice, Third EditionRating: 5 out of 5 stars5/5 (1)
- Laboratory Total Quality Management for Practitioners and Students of Medical Laboratory ScienceFrom EverandLaboratory Total Quality Management for Practitioners and Students of Medical Laboratory ScienceRating: 5 out of 5 stars5/5 (4)
- NCLEX-PN Prep Plus: 2 Practice Tests + Proven Strategies + Online + VideoFrom EverandNCLEX-PN Prep Plus: 2 Practice Tests + Proven Strategies + Online + VideoNo ratings yet
- How to Enhance Your Medical Academic Portfolio: A Guide for Doctors in TrainingFrom EverandHow to Enhance Your Medical Academic Portfolio: A Guide for Doctors in TrainingNo ratings yet
- Nursing: Scope and Standards of Practice, 4th EditionFrom EverandNursing: Scope and Standards of Practice, 4th EditionRating: 5 out of 5 stars5/5 (1)
- A Handbook for Student Nurses, 201819 edition: Introducing key issues relevant for practiceFrom EverandA Handbook for Student Nurses, 201819 edition: Introducing key issues relevant for practiceNo ratings yet
- The Art and Science of Nurse Coaching, 2nd Edition: The Provider’s Guide to Coaching Scope and Competencies, 2nd editionFrom EverandThe Art and Science of Nurse Coaching, 2nd Edition: The Provider’s Guide to Coaching Scope and Competencies, 2nd editionNo ratings yet
- Bangladesh National Nutrition Services: Assessment of Implementation StatusFrom EverandBangladesh National Nutrition Services: Assessment of Implementation StatusNo ratings yet
- Quality Assurance in Medical Education: A Practical GuideFrom EverandQuality Assurance in Medical Education: A Practical GuideNo ratings yet
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, Accreditation, and Patient SafetyFrom EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, Accreditation, and Patient SafetyNo ratings yet
- Numeracy and Clinical Calculations for Nurses, second editionFrom EverandNumeracy and Clinical Calculations for Nurses, second editionRating: 1 out of 5 stars1/5 (1)
- Implementation Guidelines For Lateral Flow Urine LipoarabinomannanDocument71 pagesImplementation Guidelines For Lateral Flow Urine LipoarabinomannantatekNo ratings yet
- Xalayaa Waamicha Hospitaala HirnaaDocument4 pagesXalayaa Waamicha Hospitaala HirnaatatekNo ratings yet
- Chapter 05Document52 pagesChapter 05tatekNo ratings yet
- Dub Deebii Komii Jijjirraa Fi Xaalayaa Waamichaa Hospitaala HoolotaaDocument14 pagesDub Deebii Komii Jijjirraa Fi Xaalayaa Waamichaa Hospitaala HoolotaatatekNo ratings yet
- PP ACF AssignmentDocument22 pagesPP ACF AssignmenttatekNo ratings yet
- Maqaa Ogeesota Digrii 1ffaa Yunversiitii Wallaggaa 2015Document18 pagesMaqaa Ogeesota Digrii 1ffaa Yunversiitii Wallaggaa 2015tatekNo ratings yet
- Komiilee Jijjiirraan Walqabatee Deebii KennameefDocument6 pagesKomiilee Jijjiirraan Walqabatee Deebii KennameeftatekNo ratings yet
- Gada Grade 2 PDFDocument33 pagesGada Grade 2 PDFtatek100% (1)
- JijjiirraDocument27 pagesJijjiirratatekNo ratings yet
- Chapter 04Document36 pagesChapter 04tatekNo ratings yet
- Hosp Fedh 1pdfDocument18 pagesHosp Fedh 1pdftatekNo ratings yet
- Feedhii Qabeenya Namaa Godinaalee Kan Bara 2014Document15 pagesFeedhii Qabeenya Namaa Godinaalee Kan Bara 2014tatekNo ratings yet
- Chapter 06Document37 pagesChapter 06tatekNo ratings yet
- Chapter 02Document36 pagesChapter 02tatekNo ratings yet
- Futures Valuation and Hedging: by Cheng Few Lee Joseph Finnerty John Lee Alice C Lee Donald WortDocument54 pagesFutures Valuation and Hedging: by Cheng Few Lee Joseph Finnerty John Lee Alice C Lee Donald WorttatekNo ratings yet
- A-01 Article ReviewDocument1 pageA-01 Article ReviewtatekNo ratings yet
- Chapter 03Document31 pagesChapter 03tatekNo ratings yet
- ADV. Cost24 MarchDocument63 pagesADV. Cost24 MarchtatekNo ratings yet
- 1243 2013 Commercial Code Proclamation No 1243 2021Document358 pages1243 2013 Commercial Code Proclamation No 1243 2021tatek100% (1)
- Afaan OromooDocument12 pagesAfaan Oromootatek100% (1)
- Strategic Implementation, Evaluation and ControllingDocument14 pagesStrategic Implementation, Evaluation and ControllingtatekNo ratings yet
- Dir.2 2004 InvestenentDocument9 pagesDir.2 2004 InvestenenttatekNo ratings yet
- Capital Budgeting Processesfor Public Sector Development Projects Master ThesisDocument65 pagesCapital Budgeting Processesfor Public Sector Development Projects Master ThesistatekNo ratings yet
- 8 MST Vol 7 No 13 Jan Jun 2017 Ayele Final Thesis For PublicationDocument21 pages8 MST Vol 7 No 13 Jan Jun 2017 Ayele Final Thesis For PublicationtatekNo ratings yet
- Proclamation No 99 2005 Rural Land Use Payment and Agricultural Activities Income Tax AmendmentDocument10 pagesProclamation No 99 2005 Rural Land Use Payment and Agricultural Activities Income Tax AmendmenttatekNo ratings yet
- Proclamation NoDocument10 pagesProclamation NotatekNo ratings yet
- Proclamation No 136 2008 Excise Tax Amendment - 2Document2 pagesProclamation No 136 2008 Excise Tax Amendment - 2tatekNo ratings yet
- 71-2004Document22 pages71-2004tatek100% (1)
- Dir - Barsiistota Yeroo Dabalata Barsisan Gibbira KaffalchisuDocument5 pagesDir - Barsiistota Yeroo Dabalata Barsisan Gibbira KaffalchisutatekNo ratings yet
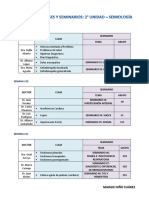
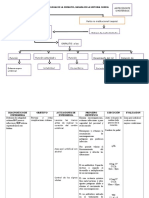
- Semiologia (Clases y Seminarios - 2° Unidad)Document3 pagesSemiologia (Clases y Seminarios - 2° Unidad)Erik QuezadaNo ratings yet
- Doctors Can Use Voice-Recognition Technology in The Operating Room To Automatically Take and Label Pictures During A ProcedureDocument2 pagesDoctors Can Use Voice-Recognition Technology in The Operating Room To Automatically Take and Label Pictures During A ProcedureSoapyNo ratings yet
- ETO NA TALAGA - Tapos Na Ang Lahat !!!Document32 pagesETO NA TALAGA - Tapos Na Ang Lahat !!!Keenen Engel Bonifacio Pascua100% (1)
- Benson Pudendal NeuralgiaDocument6 pagesBenson Pudendal NeuralgiaCronoshineNo ratings yet
- Equilibrio A-B CompletoDocument46 pagesEquilibrio A-B Completoirliana55No ratings yet
- Anestésicos Utilizados en OdontologíaDocument21 pagesAnestésicos Utilizados en OdontologíaEmmanuel Soriano Noguez100% (8)
- TanatologíaDocument8 pagesTanatologíaGaby Gabiithaa GatesNo ratings yet
- 6.estudio Previo Home Care Ipiales 2020Document111 pages6.estudio Previo Home Care Ipiales 2020Subdirección CientificaHOMRO100% (1)
- ABG AnalysisDocument15 pagesABG AnalysisPabhat Kumar100% (2)
- Reglamento Posgrado UnivalleDocument14 pagesReglamento Posgrado UnivalleHamilton DelgadoNo ratings yet
- Semana 16Document32 pagesSemana 16Williams Ramos SolisNo ratings yet
- Ug Term 20172018Document242 pagesUg Term 20172018Ooi Ban JuanNo ratings yet
- Preguntas de Diagnostico Por ImágenesDocument5 pagesPreguntas de Diagnostico Por ImágenesJoseph HSNo ratings yet
- OET Reading Test 7 - Part BDocument13 pagesOET Reading Test 7 - Part BLOTSOFTESTS80% (5)
- ANATOMIA Y RADIOLOGIA VASCULAR (Definitivo)Document18 pagesANATOMIA Y RADIOLOGIA VASCULAR (Definitivo)Carlos Arroyo AcostaNo ratings yet
- 724ccdf1 8fab 40fc Abfd Ea5ae746db97Document2 pages724ccdf1 8fab 40fc Abfd Ea5ae746db97jeronimo cordobaNo ratings yet
- OSTEOARTRITISDocument2 pagesOSTEOARTRITISNatalia Mussi Polo ArroyoNo ratings yet
- A Drug Study On: Furosemide TabletDocument7 pagesA Drug Study On: Furosemide TabletRaijenne VersolaNo ratings yet
- Oxigenoterapia y NebulizaciónDocument35 pagesOxigenoterapia y NebulizaciónYudy Andrea Castrillon Torres100% (3)
- Onfalitis Modelo CallistaDocument8 pagesOnfalitis Modelo CallistaIván MoncayoNo ratings yet
- Insuffisance Antéhypophysaire KikiDocument3 pagesInsuffisance Antéhypophysaire KikiIkram BendehbiNo ratings yet
- Epoc Caso ClinicoDocument8 pagesEpoc Caso ClinicoFranz Christian Cordova PeñaNo ratings yet
- Entrevista Con Un Médico Especialista en Herbolaria y Terapias Alternativas.Document7 pagesEntrevista Con Un Médico Especialista en Herbolaria y Terapias Alternativas.Leo DuMeNo ratings yet
- Tarea 4 Psicologia GeneralDocument2 pagesTarea 4 Psicologia GeneralKarenny 04No ratings yet
- Test Result N2gtzrg6yvDocument5 pagesTest Result N2gtzrg6yvGabiNo ratings yet
- Stool Collection Guidelines: You Will NeedDocument5 pagesStool Collection Guidelines: You Will NeedBianca Nicole Gacad FernandezNo ratings yet
- RMBI Question Bank (Solved)Document15 pagesRMBI Question Bank (Solved)AK100% (2)
- Articulo de DimensionesDocument23 pagesArticulo de DimensionesKarin A. ChiongNo ratings yet
- Public Health MODULE 7 - Pharmacists, Vaccines, and Public HealthDocument13 pagesPublic Health MODULE 7 - Pharmacists, Vaccines, and Public HealthEmerson John TallodNo ratings yet
- UW Step 2 CK Peds-Update 1Document572 pagesUW Step 2 CK Peds-Update 1Selena Gajić100% (3)