You might also like
- Skin Care PowerpointDocument52 pagesSkin Care Powerpointisapatrick812667% (3)
- 特变电工画册(英文定稿)Document52 pages特变电工画册(英文定稿)Diego MantillaNo ratings yet
- Airbus GlossaryDocument32 pagesAirbus GlossaryLuís Rodrigues100% (2)
- DR Mohit Gulati (PT)Document62 pagesDR Mohit Gulati (PT)Shubha DiwakarNo ratings yet
- Assessing and Classifying Pressure SoresDocument7 pagesAssessing and Classifying Pressure SoresAnnette Baines100% (1)
- Pressure UlcersDocument43 pagesPressure UlcersZubda Butt100% (2)
- Bed Sore 48Document45 pagesBed Sore 48Sedaka DonaldsonNo ratings yet
- Decubitus UlcerDocument14 pagesDecubitus Ulcerayman100% (3)
- Decubitus UlcerDocument30 pagesDecubitus UlcerZgama AbdulrahmanNo ratings yet
- Pressure SoresDocument20 pagesPressure SoresRupika Sodhi100% (1)
- Pressure Sore Prevention & TreatmentDocument21 pagesPressure Sore Prevention & TreatmentDrsauga France100% (1)
- Bed SoresDocument15 pagesBed Soresver_at_work100% (1)
- Pressure Ulcer CareDocument26 pagesPressure Ulcer CarekurapotaNo ratings yet
- What Is Pressure Ulcer?: Signs and SymptomsDocument6 pagesWhat Is Pressure Ulcer?: Signs and Symptomsshenecajean carajayNo ratings yet
- Pressure Sores & ManagementDocument15 pagesPressure Sores & Managementmupt77No ratings yet
- Decubitus UlcerDocument8 pagesDecubitus UlcerDanilo EspinoNo ratings yet
- Pressure Ulcer Care PresentationDocument5 pagesPressure Ulcer Care PresentationpriyaNo ratings yet
- Pressure Ulcer Prevention and TreatmentDocument51 pagesPressure Ulcer Prevention and TreatmentIosefina DudeanuNo ratings yet
- Skin Integrity and Wound Care: Types, Stages, and Risk FactorsDocument25 pagesSkin Integrity and Wound Care: Types, Stages, and Risk FactorsMitul PeterNo ratings yet
- Hips Back Ankles Buttocks HeelsDocument13 pagesHips Back Ankles Buttocks Heelsفرزدق الحسيناويNo ratings yet
- NOTES of Management of Pressure UlcersDocument4 pagesNOTES of Management of Pressure UlcersD Dimpy ThakurNo ratings yet
- Bed SoresDocument15 pagesBed SoresKhalil SalehNo ratings yet
- Decubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EDocument32 pagesDecubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EXaxa AngodNo ratings yet
- Fistuales, BedsoreDocument4 pagesFistuales, BedsoreSagar KhairwalNo ratings yet
- Wound CareDocument7 pagesWound CareAbogadie Dione Blas ReyNo ratings yet
- Unit # 06 Skin Management Insta Husain.z.kmuDocument43 pagesUnit # 06 Skin Management Insta Husain.z.kmuAamir IqbalNo ratings yet
- Types of Wounds and Phases of HealingDocument6 pagesTypes of Wounds and Phases of HealingAsniah Hadjiadatu AbdullahNo ratings yet
- Nathaniel Bed SoresDocument3 pagesNathaniel Bed Soresanon-897073No ratings yet
- Pressure UlcersDocument5 pagesPressure UlcersAmna AliNo ratings yet
- Skin IntegrityDocument112 pagesSkin IntegrityHerlina NababanNo ratings yet
- Unit 11 Skin Integrity and Wound CareDocument47 pagesUnit 11 Skin Integrity and Wound CareAshaNo ratings yet
- Skin IntegrityDocument56 pagesSkin IntegrityneehoshiNo ratings yet
- WOUND CARE and BANDAGINGDocument9 pagesWOUND CARE and BANDAGINGJane BelvisNo ratings yet
- Integu11 Pressure UlcresDocument11 pagesIntegu11 Pressure UlcresEliza ButtNo ratings yet
- Pressure Injuries: RLE Group 4: Iris Khan April Labrador Erika Lorenzana Blaise Lozano JM MatadosDocument17 pagesPressure Injuries: RLE Group 4: Iris Khan April Labrador Erika Lorenzana Blaise Lozano JM MatadosApril Mae Magos LabradorNo ratings yet
- 02 AmputationDocument23 pages02 AmputationJuanitoCabatañaLimIIINo ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- What Is BedsoresDocument4 pagesWhat Is Bedsoresver_at_workNo ratings yet
- Pressure Sores: AssessmentDocument7 pagesPressure Sores: AssessmentXyzelle Kim Monteilo OrtizNo ratings yet
- Assessing and Preventing Pressure UlcersDocument8 pagesAssessing and Preventing Pressure UlcersTamil VillardoNo ratings yet
- 06 Skin Care, Aseptic Technique and Prevention For The Pressure UlcersDocument7 pages06 Skin Care, Aseptic Technique and Prevention For The Pressure Ulcers楊畯凱No ratings yet
- 1.RagragPreventing Pressure Sore.1Document18 pages1.RagragPreventing Pressure Sore.1alsamixersNo ratings yet
- Pressure UlcerDocument66 pagesPressure UlcerSwarnkar JayeshNo ratings yet
- Pressure Ulcers: Francisco Torres Lozada MD Ponce Health Sciences University GeriatricsDocument67 pagesPressure Ulcers: Francisco Torres Lozada MD Ponce Health Sciences University GeriatricsStephanie RiveraNo ratings yet
- Pathophysiology and Prevention of Scar Tissues - NataDocument45 pagesPathophysiology and Prevention of Scar Tissues - Natadenybudiman04100% (1)
- Sistem Integumentum 2Document19 pagesSistem Integumentum 2Andrianus SudarmonoNo ratings yet
- Skin Care and Management of Pressure UlcerDocument24 pagesSkin Care and Management of Pressure UlcerchellczyNo ratings yet
- Pressure Ulcer Care Guide: Stages, Treatments & Nursing InterventionsDocument39 pagesPressure Ulcer Care Guide: Stages, Treatments & Nursing InterventionsRosalyn YuNo ratings yet
- Bali Geriatric Symposium 2018 UpdateDocument40 pagesBali Geriatric Symposium 2018 UpdateMardikaNo ratings yet
- 3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsDocument12 pages3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsJOSHUA DICHOSONo ratings yet
- Pressure Ulcers SimplifiedDocument8 pagesPressure Ulcers SimplifiedMsPocketbook HoarderNo ratings yet
- Wound ManagementDocument72 pagesWound Managementdrsonuchawla100% (1)
- Necrotizing FasciitisDocument11 pagesNecrotizing FasciitisElvira Rodriguez EstebanNo ratings yet
- Tissue Integrity Outline Spring 2023Document25 pagesTissue Integrity Outline Spring 2023morganstorey0No ratings yet
- 4.wound Care IDocument46 pages4.wound Care Iamir aizatNo ratings yet
- Skin and Pressure SoresDocument24 pagesSkin and Pressure SoresJennyNo ratings yet
- Pressure UlcersDocument38 pagesPressure UlcersRadwa EbedNo ratings yet
- Guide to Acute, Chronic Wounds: Types, Causes, HealingDocument4 pagesGuide to Acute, Chronic Wounds: Types, Causes, HealingBayu Mario GintingNo ratings yet
- Venous Ulcer Treatment GuideDocument41 pagesVenous Ulcer Treatment GuideLAL DIME 1No ratings yet
- 2 Skin-IntegrityDocument74 pages2 Skin-IntegrityFlourence ZafranNo ratings yet
- Open Fracture Classification and TreatmentDocument70 pagesOpen Fracture Classification and TreatmentKelly Khesya100% (1)
- Interview Questions - Godrej Technical & HR Interview QuestionsDocument9 pagesInterview Questions - Godrej Technical & HR Interview Questionssasithar jaisankaranNo ratings yet
- Namma Kalvi 12th Maths Book Back 1 Mark Questions em 216251Document29 pagesNamma Kalvi 12th Maths Book Back 1 Mark Questions em 21625111B CHARAN ANANDNo ratings yet
- Review of oxidative stress and antioxidants in dentistryDocument4 pagesReview of oxidative stress and antioxidants in dentistrySeeptianMaulanaNo ratings yet
- Ase Utra Military and Law Enforcement ProductsDocument12 pagesAse Utra Military and Law Enforcement ProductsjamesfletcherNo ratings yet
- Small Cells 2013 BrochuresDocument22 pagesSmall Cells 2013 BrochuresChungwa ChanjiNo ratings yet
- Ic F3022SDocument36 pagesIc F3022SEfren.galNo ratings yet
- The Volcanic Explosivity Index (VEI)Document8 pagesThe Volcanic Explosivity Index (VEI)Rakhmatul ArafatNo ratings yet
- 5 Commandments of DatingDocument8 pages5 Commandments of DatingBariki MwasagaNo ratings yet
- OK - EndUserGuideHoseSafetyInstituteDocument8 pagesOK - EndUserGuideHoseSafetyInstituteSunil GhosalkarNo ratings yet
- Chapter11 Part1 PDFDocument40 pagesChapter11 Part1 PDFvampanezezNo ratings yet
- 52 Blower StoryDocument7 pages52 Blower StoryBentley SpottingNo ratings yet
- Basic Integration Problems #1Document4 pagesBasic Integration Problems #1John Marlo GorobaoNo ratings yet
- Fox em Corporate Presentation 08 2022Document19 pagesFox em Corporate Presentation 08 2022Pierluigi GhioneNo ratings yet
- Environmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesDocument27 pagesEnvironmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesLaraNo ratings yet
- Beira Port MozambiqueDocument4 pagesBeira Port Mozambiqueripper_oopsNo ratings yet
- 8-Input Multiplexer Selects One of Eight InputsDocument3 pages8-Input Multiplexer Selects One of Eight InputsKang RoyNo ratings yet
- 17 The Tarrying TimeDocument22 pages17 The Tarrying Timeapi-303147801100% (1)
- Vdocuments - MX - Control Systems by Nagrath Gopal Solution Manual PDFDocument128 pagesVdocuments - MX - Control Systems by Nagrath Gopal Solution Manual PDFPriyadarshini SahooNo ratings yet
- 85 KW RequestDocument3 pages85 KW Requestاختر بلوچNo ratings yet
- Week 05 - Mechanical Properties Part 1Document48 pagesWeek 05 - Mechanical Properties Part 1Dharshica MohanNo ratings yet
- Pol Science ProjectDocument18 pagesPol Science ProjectAnshu SharmaNo ratings yet
- All Questions SLDocument50 pagesAll Questions SLRoberto Javier Vázquez MenchacaNo ratings yet
- Home Automation Chapter 1Document7 pagesHome Automation Chapter 1Nishant Sawant100% (1)
- Mushroom Umami Taste EvaluationDocument10 pagesMushroom Umami Taste EvaluationMaryam HanifNo ratings yet
- Mixed Use DevelopmentDocument3 pagesMixed Use DevelopmentMark Darcy UngsonNo ratings yet
- DSBV87ALP Two-Stage Differential Pressure Control Valve SpecsDocument2 pagesDSBV87ALP Two-Stage Differential Pressure Control Valve SpecsadrianioantomaNo ratings yet
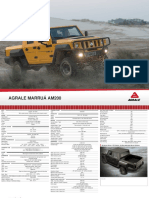
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet