You might also like
- Assessing and Preventing Pressure UlcersDocument8 pagesAssessing and Preventing Pressure UlcersTamil VillardoNo ratings yet
- Pressure Ulcers: Jorge G. Ruiz, MD, FACPDocument71 pagesPressure Ulcers: Jorge G. Ruiz, MD, FACPRomilPatelNo ratings yet
- Nursing Intervention Plan for Fracture PatientDocument2 pagesNursing Intervention Plan for Fracture PatientAce Dioso TubascoNo ratings yet
- Grade 8 BowDocument7 pagesGrade 8 BowJorely Barbero MundaNo ratings yet
- Study Skills GroupDocument25 pagesStudy Skills Groupapi-654376760No ratings yet
- Preventing Skin Damage and Pressure UlcersDocument29 pagesPreventing Skin Damage and Pressure UlcersJOSHUA DICHOSO100% (1)
- CVA Impaired Physical MobilityDocument3 pagesCVA Impaired Physical MobilityJasmineNo ratings yet
- Impaired Physical Mobility Related To Application of Traction or Cast As Evidenced by AssessmentDocument13 pagesImpaired Physical Mobility Related To Application of Traction or Cast As Evidenced by AssessmentJaylord VerazonNo ratings yet
- Heart Failure COncept MapDocument2 pagesHeart Failure COncept MapJrBong SemaneroNo ratings yet
- Nursing Care Plans Made EasyDocument23 pagesNursing Care Plans Made EasyJOSHUA DICHOSONo ratings yet
- Impaired MobilityDocument3 pagesImpaired MobilityYeana AlonNo ratings yet
- Patient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)Document28 pagesPatient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)JOSHUA DICHOSO100% (1)
- Communication in Marriage Reed 105Document28 pagesCommunication in Marriage Reed 105Erwin Y. CabaronNo ratings yet
- Risk For InfectionDocument3 pagesRisk For Infectionprickybiik100% (1)
- Welfare Services For Challenged ChildrenDocument42 pagesWelfare Services For Challenged ChildrenRahul Dhaker70% (10)
- 4 Amputation Nursing Care Plans - Nurseslabs-1 PDFDocument12 pages4 Amputation Nursing Care Plans - Nurseslabs-1 PDFsaidi MwanamongaNo ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- Concept Map PEDocument3 pagesConcept Map PERobert MariasiNo ratings yet
- Nursing Care Plan for Self-Care DeficitDocument3 pagesNursing Care Plan for Self-Care DeficitSteph_Toinkz_240No ratings yet
- NCP Impaired SkinDocument3 pagesNCP Impaired SkinRuby AnneNo ratings yet
- Nursing Care Plan Risk For Infection OB University of Santo Tomas College of NursingDocument2 pagesNursing Care Plan Risk For Infection OB University of Santo Tomas College of NursingKaren ValdezNo ratings yet
- ABM Applied Economics Module 2 Examine The Utility and Application of of Applied Economics To Solve Economic Issues and ProblemsDocument29 pagesABM Applied Economics Module 2 Examine The Utility and Application of of Applied Economics To Solve Economic Issues and Problemsmara ellyn lacson100% (8)
- Impaired Skin Integrity Related To Inflammatory Response Secondary To InfectionDocument7 pagesImpaired Skin Integrity Related To Inflammatory Response Secondary To InfectionyammyouNo ratings yet
- Stage 1 Overcoming Imposter Syndrome: What You Will LearnDocument4 pagesStage 1 Overcoming Imposter Syndrome: What You Will LearnPaul Ioan PopescuNo ratings yet
- Cebu Normal University College of Nursing Center of Excellence Level IV Re-Accredited Drug StudyDocument5 pagesCebu Normal University College of Nursing Center of Excellence Level IV Re-Accredited Drug StudyChelsea WuNo ratings yet
- Mirko Workout PDFDocument10 pagesMirko Workout PDFSirine Boussama100% (3)
- NCP: FracturesDocument21 pagesNCP: FracturesJavie100% (1)
- Risk For Aspiration Related To Impaired Swallowing Secondary To Cerebrovascular AccidentDocument3 pagesRisk For Aspiration Related To Impaired Swallowing Secondary To Cerebrovascular AccidentChenee MabulayNo ratings yet
- Fracture Nursing CareDocument6 pagesFracture Nursing CareRizqi LutfiNo ratings yet
- NCP - Impaired Skin IntegrityDocument3 pagesNCP - Impaired Skin IntegrityFlauros Ryu Jabien90% (29)
- Nursing Care PlansDocument3 pagesNursing Care PlansBeyotchsangreMesswithurownlifeNo ratings yet
- NCP1 CHFDocument2 pagesNCP1 CHFapi-27015740100% (5)
- Do Genes Determine Champions?Document6 pagesDo Genes Determine Champions?mensrea0No ratings yet
- Feasibility Study 1Document69 pagesFeasibility Study 1Andre Christian Ang100% (2)
- Or Write Up 52611Document14 pagesOr Write Up 52611babydumplingsNo ratings yet
- Day 3 Activity: Nursing Care Plan: College of Health SciencesDocument6 pagesDay 3 Activity: Nursing Care Plan: College of Health SciencesAngelica Charisse BuliganNo ratings yet
- Cues Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument19 pagesCues Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationEmeEmeka100% (1)
- NCP OrifDocument8 pagesNCP Orif2211890001No ratings yet
- NCP: Patient With A Pressure UlcerDocument2 pagesNCP: Patient With A Pressure UlcerICa MarlinaNo ratings yet
- NCP TahbsoDocument18 pagesNCP TahbsoKe EjieNo ratings yet
- Kawasaki Disease-Case-Study LATEST CHANGESDocument24 pagesKawasaki Disease-Case-Study LATEST CHANGESJesse James Advincula Edjec100% (7)
- Nursing Care Plan-1idealDocument30 pagesNursing Care Plan-1idealSheila Mae PanisNo ratings yet
- NCPDocument7 pagesNCPMarius Clifford BilledoNo ratings yet
- Nursing Care Plan Infection)Document4 pagesNursing Care Plan Infection)Kez Domine100% (1)
- Introduction To Pharmaceutical MicrobiologyDocument35 pagesIntroduction To Pharmaceutical MicrobiologylorrainebarandonNo ratings yet
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDocument4 pagesCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- LFD CommunityDocument2 pagesLFD CommunityJanry-Mae Escobar TumanengNo ratings yet
- Cva NCPDocument2 pagesCva NCPAkima Mulok0% (1)
- ImmobilityDocument1 pageImmobilitymicopoliNo ratings yet
- Lacerated WoundDocument38 pagesLacerated Wounddomzlr18100% (2)
- Reaction Paper ERDocument1 pageReaction Paper ERVann Anthony FuentesNo ratings yet
- Drug Study EditedDocument5 pagesDrug Study EditedfabtaciousVeelaNo ratings yet
- NCP SicuDocument6 pagesNCP SicuChoco MuchoNo ratings yet
- AcetaminophenDocument3 pagesAcetaminophenShaira Tan100% (1)
- Surgical NCPDocument6 pagesSurgical NCPAreeya SushmitaNo ratings yet
- Risk For SuicideDocument3 pagesRisk For SuicidepamfiestaNo ratings yet
- Acute Pain Prioritization After HysterectomyDocument2 pagesAcute Pain Prioritization After HysterectomyRuth Lea Cabrera100% (1)
- LevofloxacinDocument15 pagesLevofloxacinsonal aranhaNo ratings yet
- Guaifenesin Drug CardDocument1 pageGuaifenesin Drug CardJessie JenningsNo ratings yet
- Nursing Informatics - Information Security and ConfidentialityDocument5 pagesNursing Informatics - Information Security and ConfidentialityReya Seno100% (1)
- NCP Self Care DeficitDocument3 pagesNCP Self Care DeficitLeizel ApolonioNo ratings yet
- NCP Skin IntegityDocument3 pagesNCP Skin Integityclydell joyce masiarNo ratings yet
- Date and Time: Nursing Care Plan (NCP)Document3 pagesDate and Time: Nursing Care Plan (NCP)Deanne Carla DalilisNo ratings yet
- Risk For Fall and Risk For Imbalanced Nutrition Less Than Body Requirements Pantoprazole, Ketorolac, Cefoxitin Drug StudyDocument4 pagesRisk For Fall and Risk For Imbalanced Nutrition Less Than Body Requirements Pantoprazole, Ketorolac, Cefoxitin Drug StudyKevin John ReaLubit SaLisiNo ratings yet
- Nursing Care Plan CVADocument6 pagesNursing Care Plan CVAessevyNo ratings yet
- Self Task For English Lesson Part 2THDocument1 pageSelf Task For English Lesson Part 2THistiningrum0% (1)
- Drug Study - CaDocument3 pagesDrug Study - Casaint_ronald8No ratings yet
- BSN 215 Reflection Essay - LagoDocument2 pagesBSN 215 Reflection Essay - LagoAlliahkherzteen LagoNo ratings yet
- NANDA Definition:: Ongoing AssessmentDocument3 pagesNANDA Definition:: Ongoing AssessmentKat LazoNo ratings yet
- Nurses Role in Care & Prevention of PressureDocument25 pagesNurses Role in Care & Prevention of PressureLinda andayaniNo ratings yet
- Pressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisDocument7 pagesPressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisAlexis TrivinoNo ratings yet
- Assessing Risk of Pressure UlcersDocument2 pagesAssessing Risk of Pressure Ulcerscrystal_rc9No ratings yet
- Bedsores: Eligrace F. Fabian, RNDocument22 pagesBedsores: Eligrace F. Fabian, RNsweetsai05No ratings yet
- GE 8 Ethics PESTLE AnalysisDocument3 pagesGE 8 Ethics PESTLE AnalysisJOSHUA DICHOSONo ratings yet
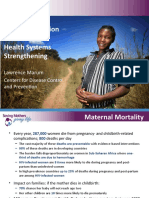
- Blood Transfusion Services Strengthen Maternal HealthDocument19 pagesBlood Transfusion Services Strengthen Maternal HealthJOSHUA DICHOSONo ratings yet
- Advances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVDocument19 pagesAdvances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVJOSHUA DICHOSONo ratings yet
- Case PresentationDocument39 pagesCase PresentationJOSHUA DICHOSONo ratings yet
- Pneumonia Presenting as Acute Abdomen in ChildrenDocument4 pagesPneumonia Presenting as Acute Abdomen in ChildrenJOSHUA DICHOSONo ratings yet
- CHN ConceptsDocument48 pagesCHN ConceptsJOSHUA DICHOSONo ratings yet
- Philippines Commitment Self-Reporting Questionnaire 2018Document7 pagesPhilippines Commitment Self-Reporting Questionnaire 2018JOSHUA DICHOSONo ratings yet
- (.-..-.)Document1 page(.-..-.)JOSHUA DICHOSONo ratings yet
- Case Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesDocument2 pagesCase Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesJOSHUA DICHOSONo ratings yet
- Which of The Statements Explains The Saying "All Work and No Play Make Jack A Dull Boy." 2 PointsDocument2 pagesWhich of The Statements Explains The Saying "All Work and No Play Make Jack A Dull Boy." 2 PointsJOSHUA DICHOSONo ratings yet
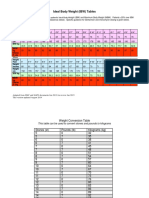
- IBW TableDocument2 pagesIBW TablegrafikeyesNo ratings yet
- 6234-Article Text-8420-2-10-20170221Document3 pages6234-Article Text-8420-2-10-20170221Jenry Himawan SinagaNo ratings yet
- Recommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseDocument34 pagesRecommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseJOSHUA DICHOSONo ratings yet
- P롶허ㅓㅠㄹ포ㅗ)Document19 pagesP롶허ㅓㅠㄹ포ㅗ)JOSHUA DICHOSONo ratings yet
- Nursing Interventions and Rationales - Impaired Skin IntegrityDocument11 pagesNursing Interventions and Rationales - Impaired Skin IntegrityJOSHUA DICHOSONo ratings yet
- Case Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesDocument2 pagesCase Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesJOSHUA DICHOSONo ratings yet
- Physiological Rationale and Current Evidence For Therapeutic Positioning of Critically Ill Patients PDFDocument15 pagesPhysiological Rationale and Current Evidence For Therapeutic Positioning of Critically Ill Patients PDFnurulanisa0703No ratings yet
- How To Study Pharmacology Checklist Cheat SheetDocument4 pagesHow To Study Pharmacology Checklist Cheat SheetJOSHUA DICHOSONo ratings yet
- Advances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVDocument19 pagesAdvances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVJOSHUA DICHOSONo ratings yet
- Introduction PDFDocument1 pageIntroduction PDFJOSHUA DICHOSONo ratings yet
- De Nition: Chapter 46 Chest ExaminationDocument7 pagesDe Nition: Chapter 46 Chest ExaminationJOSHUA DICHOSONo ratings yet
- Tobacco Use and Second-Hand Smoke Exposure in Pregnancy: WHO RecommendationsDocument104 pagesTobacco Use and Second-Hand Smoke Exposure in Pregnancy: WHO RecommendationsJOSHUA DICHOSONo ratings yet
- Agency Visit Bureau of Fire Protection Sorsogon City: Joshua C. Dichoso 1BSN3Document2 pagesAgency Visit Bureau of Fire Protection Sorsogon City: Joshua C. Dichoso 1BSN3JOSHUA DICHOSONo ratings yet
- Course Syllabus: Course: Hours: Course DescriptionDocument10 pagesCourse Syllabus: Course: Hours: Course DescriptionJOSHUA DICHOSONo ratings yet
- Distraction Techniques For Face and Smile Aesthetic Preventing Ageing DecayDocument10 pagesDistraction Techniques For Face and Smile Aesthetic Preventing Ageing DecayAarónNo ratings yet
- Declaration of James Sheldon2318Document7 pagesDeclaration of James Sheldon2318James Sheldon Jr.No ratings yet
- Chrome Lignosulfonate (CLS)Document5 pagesChrome Lignosulfonate (CLS)sajad gohariNo ratings yet
- ACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESDocument10 pagesACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESYanti TandjungNo ratings yet
- CEMP-Framework Beach Project Scope Rev0Document152 pagesCEMP-Framework Beach Project Scope Rev0gowthamNo ratings yet
- HR Selection Process & Global PerspectivesDocument30 pagesHR Selection Process & Global PerspectivesOsei Kwame PhilipNo ratings yet
- Adherence To Nucleos (T) Ide Analogue PDFDocument8 pagesAdherence To Nucleos (T) Ide Analogue PDFVirgo WNo ratings yet
- Pool Paint Safety Data SheetDocument9 pagesPool Paint Safety Data SheetNicholson Vhenz UyNo ratings yet
- Tool Box Talk - MK - Emergency Response ProceduresDocument2 pagesTool Box Talk - MK - Emergency Response ProceduresPaul McGahanNo ratings yet
- CrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)Document5 pagesCrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)TUTOR PAULO EDUARDO REDKVANo ratings yet
- Sports Medicine 10-Lesson 4 - Lower Leg Muscles Turf ToeDocument5 pagesSports Medicine 10-Lesson 4 - Lower Leg Muscles Turf Toeapi-383568582No ratings yet
- Middle East CaravanDocument20 pagesMiddle East CaravanB2B AFRICANo ratings yet
- MCN ReviewerDocument3 pagesMCN ReviewerJunghoon YangParkNo ratings yet
- MSDS DDDocument2 pagesMSDS DDBaher SaidNo ratings yet
- Chapter Two-Foundation of Individual Behavior and Learning in An OrganizationDocument16 pagesChapter Two-Foundation of Individual Behavior and Learning in An OrganizationMikias DegwaleNo ratings yet
- Essential Falls Management Series: Managing Falls in Assisted Living (Tideiksaar Excerpt)Document11 pagesEssential Falls Management Series: Managing Falls in Assisted Living (Tideiksaar Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.No ratings yet
- Proficiency Test 7-6-2021Document23 pagesProficiency Test 7-6-2021Thịnh Hoàng MinhNo ratings yet
- قواعد التوثيق في البحوث والدراسات التربويةDocument19 pagesقواعد التوثيق في البحوث والدراسات التربويةnemra1No ratings yet
- Indian EthosDocument19 pagesIndian Ethosshahid veettil100% (2)
- Use Bloom's Taxonomy to Achieve Learning GoalsDocument61 pagesUse Bloom's Taxonomy to Achieve Learning GoalsSouvik DasNo ratings yet
- Nursing Leadership Roles ResponsibilitiesDocument2 pagesNursing Leadership Roles ResponsibilitiesDan Dan ManaoisNo ratings yet