You might also like
- Clinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsFrom EverandClinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Livercirrhosisl 090306011045 Phpapp01Document38 pagesLivercirrhosisl 090306011045 Phpapp01chardz041591No ratings yet
- Pathophysiology On Liver CirrhosisDocument38 pagesPathophysiology On Liver CirrhosisYogi AnjasmaraNo ratings yet
- Pathophysiology On Liver CirrhosisDocument39 pagesPathophysiology On Liver CirrhosisswaraNo ratings yet
- Cirrhosis of LiverDocument106 pagesCirrhosis of LiveraahadNo ratings yet
- Not Activity No. 7Document12 pagesNot Activity No. 7Patricia Marie Laman YadaoNo ratings yet
- Liver Cirrhosis Paper PresentationDocument52 pagesLiver Cirrhosis Paper PresentationNagabharana Hm HollattiNo ratings yet
- MS AddsDocument4 pagesMS Addsapi-3731294No ratings yet
- Pathophysiology On Liver CirrhosisDocument38 pagesPathophysiology On Liver Cirrhosisတမန္ေတာ္ တမန္ေတာ္100% (30)
- Hypovolemic Shock PathophysiologyDocument8 pagesHypovolemic Shock PathophysiologyKAYCEENo ratings yet
- Liver CirrohosisDocument157 pagesLiver CirrohosisSeema SachdevaNo ratings yet
- 4 Accesory Organ DisordersDocument14 pages4 Accesory Organ DisordersNica EnriquezNo ratings yet
- Pathophysiology in Liver CirrhosisDocument4 pagesPathophysiology in Liver CirrhosisCyrus Ortalla RobinNo ratings yet
- Cirrhosis Copy FINAL EDITEDDocument42 pagesCirrhosis Copy FINAL EDITEDpraisidNo ratings yet
- PathoDocument7 pagesPathoAnonymous 87fNoO2fhVNo ratings yet
- Complications: Acute PancreatitisDocument2 pagesComplications: Acute PancreatitisNikey LimNo ratings yet
- 3.acute Liver Failure Without AudioDocument42 pages3.acute Liver Failure Without AudioMohamed ElkadyNo ratings yet
- MetabolismDocument39 pagesMetabolismTiffany KnepperNo ratings yet
- Medicine 1Document114 pagesMedicine 1Prajwal P ShetNo ratings yet
- Renal SystemDocument20 pagesRenal SystemRahul DasNo ratings yet
- Liver CADocument1 pageLiver CAJenny MananesNo ratings yet
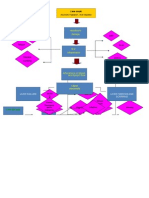
- Patofisiologi: Risiko Gangguan Nutrisi Gangguan Perfusi Jaringan Gangguan Intoleransi Aktivitas Integritas KulitDocument1 pagePatofisiologi: Risiko Gangguan Nutrisi Gangguan Perfusi Jaringan Gangguan Intoleransi Aktivitas Integritas KulitRutDanNo ratings yet
- Pa Tho Physiology Final DMDocument6 pagesPa Tho Physiology Final DMJamil LorcaNo ratings yet
- Clinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesDocument27 pagesClinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesradhiinathahirNo ratings yet
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87No ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- WOC CKD NewDocument1 pageWOC CKD Newaris novenNo ratings yet
- Trans Hepatobiliary SystemDocument5 pagesTrans Hepatobiliary SystemJulie CatianNo ratings yet
- Kidney Disorders Final PresentationDocument20 pagesKidney Disorders Final PresentationElla PaezNo ratings yet
- Cirrhosis Hepatic: DinadewisliDocument47 pagesCirrhosis Hepatic: DinadewisliwilmaNo ratings yet
- Urek UrekDocument7 pagesUrek Urekjauharotun nafisahNo ratings yet
- Viral HepatitisDocument7 pagesViral Hepatitisadrian kristopher dela cruzNo ratings yet
- AsKep - GGK Meri Punya Terbaru BGTDocument24 pagesAsKep - GGK Meri Punya Terbaru BGTAnonymous nhZCowNo ratings yet
- Final CC EdemaDocument31 pagesFinal CC EdematabatchNo ratings yet
- A ESRDDocument21 pagesA ESRDShetal SharmaNo ratings yet
- Askep SirosisDocument73 pagesAskep SirosisRisma Yuliana PratiwiNo ratings yet
- Pathway CKDDocument2 pagesPathway CKDWijayea PunkrockNo ratings yet
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Document72 pagesWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Darin MonerNo ratings yet
- 74 Acute Renal Failure UpdatedDocument48 pages74 Acute Renal Failure UpdatedaweleNo ratings yet
- Etiologies of Chronic Liver Disease: Infections, Esp. Viral Toxins Genetic Drugs Autoimmune Vascular BiliaryDocument36 pagesEtiologies of Chronic Liver Disease: Infections, Esp. Viral Toxins Genetic Drugs Autoimmune Vascular BiliaryDini Permata SariNo ratings yet
- Chronic Kidney Disease: A Great E-Guide To CKDDocument15 pagesChronic Kidney Disease: A Great E-Guide To CKDshirley_ling_15No ratings yet
- Complications of CirrhosisDocument2 pagesComplications of CirrhosisDanielle DiorioNo ratings yet
- 2-Liver DiseasesDocument28 pages2-Liver DiseasesAhmed IsmaillNo ratings yet
- 1.2.4 Web of Caution Chronic Kidney Disease (CKD)Document1 page1.2.4 Web of Caution Chronic Kidney Disease (CKD)Siska Maya SariNo ratings yet
- Patofisiologi: Kerusakan Integritas KulitDocument1 pagePatofisiologi: Kerusakan Integritas KulitAditya PratamaNo ratings yet
- Gastrointestinal Tract Bleeding: Dr. Mabel Sihombing, Sppd-KgehDocument46 pagesGastrointestinal Tract Bleeding: Dr. Mabel Sihombing, Sppd-KgehSyarifah FauziahNo ratings yet
- Sirosis HepatisDocument65 pagesSirosis HepatisIntania Fadilla100% (1)
- Acute Kidney Injury: Ahmad Fariz Malvi Zamzam ZeinDocument30 pagesAcute Kidney Injury: Ahmad Fariz Malvi Zamzam ZeinFatwa Dea Ramdani OctaviyasminNo ratings yet
- Upper Gastrointestinal Haemorrhage: S5 Unit 2006 Mbbs Batch Trivandrum Medical CollegeDocument194 pagesUpper Gastrointestinal Haemorrhage: S5 Unit 2006 Mbbs Batch Trivandrum Medical CollegeSrini VasanNo ratings yet
- 14-GIT and LiverDocument36 pages14-GIT and LiverRodriguez Vivanco Kevin DanielNo ratings yet
- Terapi Sirosis HatiDocument40 pagesTerapi Sirosis HatiRisydaMKhNo ratings yet
- 7-Kidney FunctionDocument18 pages7-Kidney FunctionAsad ullahNo ratings yet
- Medical Surgical Nursing 2 Denn Hill RiorosoDocument10 pagesMedical Surgical Nursing 2 Denn Hill RiorosoLienyPerasNo ratings yet
- Electrolyte Disorders: Crisbert I. Cualteros, MD S.page - TLDocument45 pagesElectrolyte Disorders: Crisbert I. Cualteros, MD S.page - TLm_arianne268932No ratings yet
- 2nd Year-Typical Cases To Complement PBL Scenarios 2008-09Document2 pages2nd Year-Typical Cases To Complement PBL Scenarios 2008-09trisarahtops1No ratings yet
- 6 Med Ward (WK - 1) PathophysiologyDocument3 pages6 Med Ward (WK - 1) PathophysiologyZaijean Kate Dianne LigutomNo ratings yet
- Sirosis Hepatis-Dikonversi-DikompresiDocument22 pagesSirosis Hepatis-Dikonversi-DikompresiAa SsNo ratings yet
- Cholelithiasis CholecystitisDocument1 pageCholelithiasis Cholecystitissamliebareng77No ratings yet
- Respiratory DR Osama MahmoudpdfDocument91 pagesRespiratory DR Osama MahmoudpdfGhada ElsayedNo ratings yet
- Elios Omœopathy: AB G T HDocument28 pagesElios Omœopathy: AB G T HAlberto Garcia100% (8)
- Tachdjian's Pediatric Orthopaedics v.4Document660 pagesTachdjian's Pediatric Orthopaedics v.4Leonardo Garay QuinteroNo ratings yet
- A Client With Osteoarthritis: Nursing Care PlanDocument1 pageA Client With Osteoarthritis: Nursing Care PlangeeDeeeeNo ratings yet
- A Worn Path-Eudora WeltyDocument3 pagesA Worn Path-Eudora WeltyShalini KanganNo ratings yet
- Maharashtra Cyber SecurityDocument20 pagesMaharashtra Cyber Securityimoon technologiesNo ratings yet
- Illnesses in Gilded Age and Progressive EraDocument3 pagesIllnesses in Gilded Age and Progressive EraminahilNo ratings yet
- Implants in Diabetic PatientsDocument6 pagesImplants in Diabetic PatientsSilvia SoareNo ratings yet
- Special Pathology Viva Questions by AMS 46Document32 pagesSpecial Pathology Viva Questions by AMS 46Mohan Dass100% (1)
- Sources of Nutrients and Deficiency DiseasesDocument4 pagesSources of Nutrients and Deficiency DiseasesAditya A Strange PersonNo ratings yet
- Cardiac ArrestDocument19 pagesCardiac ArrestHaimelien De LimosNo ratings yet
- Alternative Systems of MedicineDocument53 pagesAlternative Systems of MedicineShruti Baid BafnaNo ratings yet
- Oils, Blends & Products Recommended:: Reflexology PointsDocument2 pagesOils, Blends & Products Recommended:: Reflexology Pointshmaddy3117No ratings yet
- Endodontics FinalDocument114 pagesEndodontics FinalContas AleatóriasNo ratings yet
- Bams KriyakalaDocument69 pagesBams KriyakalaBalkrishan SevatkarNo ratings yet
- Demam Jonathan TandajuDocument19 pagesDemam Jonathan TandajuDessy DsyNo ratings yet
- HEALTH PROGRAMS CompleteDocument194 pagesHEALTH PROGRAMS CompleteAbigail AnziaNo ratings yet
- The 4th Dimension of FitnessDocument6 pagesThe 4th Dimension of FitnessalmaformaNo ratings yet
- Drug StudyDocument3 pagesDrug StudyLarah Mae AndogNo ratings yet
- 1.1 - Staph AureusDocument22 pages1.1 - Staph Aureusrazgriz1100% (1)
- Grow Taller 4 IdiotsDocument2 pagesGrow Taller 4 Idiotsaamlliaange0% (1)
- Introduction To Behavioral Medicine For Mental Health CounselorsDocument28 pagesIntroduction To Behavioral Medicine For Mental Health CounselorsDeva ChiruNo ratings yet
- Kuliah Mikrobiologi Bakteri Coccus Gram Positif - DR Lely SaptawatiDocument59 pagesKuliah Mikrobiologi Bakteri Coccus Gram Positif - DR Lely SaptawatiAyatiNo ratings yet
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- Daun PDFDocument5 pagesDaun PDFDaniel OktavianusNo ratings yet
- Esophageal CancerDocument42 pagesEsophageal Cancerapi-1964133750% (2)
- Uses of The Different Parts of The Neem PlantDocument7 pagesUses of The Different Parts of The Neem PlantMuthu KumarNo ratings yet
- Anaesthesia LecDocument9 pagesAnaesthesia LecVictoria CharlesworthNo ratings yet
- Summary of Anxiety Disorders (DSM-5)Document6 pagesSummary of Anxiety Disorders (DSM-5)Villamorchard100% (3)
- 10 Drug StudyDocument25 pages10 Drug StudyM AnnNo ratings yet