You might also like
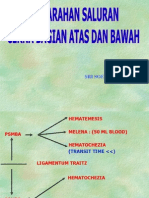
- Perdarahan Saluran Cerna Atas Dan BawahDocument34 pagesPerdarahan Saluran Cerna Atas Dan BawahKharisma PrabowoNo ratings yet
- Upper Gastrointestinal Haemorrhage: S5 Unit 2006 Mbbs Batch Trivandrum Medical CollegeDocument194 pagesUpper Gastrointestinal Haemorrhage: S5 Unit 2006 Mbbs Batch Trivandrum Medical CollegeSrini VasanNo ratings yet
- CASE 1 Group 2 7 1Document4 pagesCASE 1 Group 2 7 1Monique BorresNo ratings yet
- Upper Gastrointestinal Bleeding 4 Juni 2009Document36 pagesUpper Gastrointestinal Bleeding 4 Juni 2009YennySuryaniNo ratings yet
- Treatment and Complications of Chronic Liver DiseaseDocument40 pagesTreatment and Complications of Chronic Liver DiseaseRisydaMKhNo ratings yet
- Docc NotesDocument4 pagesDocc Noteslovegoodluna812No ratings yet
- Acute Pancreatitis: Simmedic UKMDocument28 pagesAcute Pancreatitis: Simmedic UKMRadhika PrabhuNo ratings yet
- Causes and Diagnosis of Lower Gastrointestinal BleedingDocument23 pagesCauses and Diagnosis of Lower Gastrointestinal BleedingSarachanda SallyNo ratings yet
- Upper Gi BleedingDocument37 pagesUpper Gi Bleedingfathima AlfasNo ratings yet
- Medicine 1Document114 pagesMedicine 1Prajwal P ShetNo ratings yet
- GI BleedDocument28 pagesGI BleedAnn Lan100% (1)
- Gastrointestinal Bleeding Causes and ManagementDocument36 pagesGastrointestinal Bleeding Causes and ManagementMuwanga faizoNo ratings yet
- Causes and treatment of gastrointestinal bleeding in childrenDocument21 pagesCauses and treatment of gastrointestinal bleeding in childrenAmalia Hendar PangestutiNo ratings yet
- Gi Case Study (Sep Batch)Document45 pagesGi Case Study (Sep Batch)MOHANTA, deviprasadNo ratings yet
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87No ratings yet
- Management of Upper GI BleedingDocument40 pagesManagement of Upper GI BleedingManeesha KhalseNo ratings yet
- Esophageal Varices Causes Symptoms ManagementDocument2 pagesEsophageal Varices Causes Symptoms ManagementSureen Regular100% (1)
- Upper GI BleedingDocument6 pagesUpper GI BleedingMarie Jennifer ParilNo ratings yet
- SRI SOETADI HEMORRHAGE GUIDEDocument34 pagesSRI SOETADI HEMORRHAGE GUIDETia AriantiNo ratings yet
- CME Upper GI BleedDocument46 pagesCME Upper GI Bleedfarah fadzilNo ratings yet
- Acute Pancreatitis 3rd YearDocument13 pagesAcute Pancreatitis 3rd YearAyesha FatimaNo ratings yet
- GI Bleeding - Acute PancreatitisDocument67 pagesGI Bleeding - Acute PancreatitisandikaisnaeniNo ratings yet
- Upper Gi BleedingDocument35 pagesUpper Gi BleedingAnggreini Susanti100% (2)
- Cholecystitis (Surgery)Document100 pagesCholecystitis (Surgery)Hazel Aspera100% (1)
- Acute Mesenteric Ischemia Diagnosis and ManagementDocument52 pagesAcute Mesenteric Ischemia Diagnosis and ManagementMariam ShamعaNo ratings yet
- UPPER GASTROINTESTINAL BLEEDING Simp HemoroidDocument44 pagesUPPER GASTROINTESTINAL BLEEDING Simp HemoroidKomang YudaNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Upper GI Bleed by Wajid MunirDocument49 pagesUpper GI Bleed by Wajid MunirAtifNo ratings yet
- Ascites PresentationDocument19 pagesAscites PresentationDanielle FosterNo ratings yet
- Abd Distension & Ascites-1, All NewDocument34 pagesAbd Distension & Ascites-1, All NewANENA RHODANo ratings yet
- CHOLECYSTITISDocument6 pagesCHOLECYSTITISAnar ChuluunNo ratings yet
- Acute Gi Bleeding: Rohman AzzamDocument34 pagesAcute Gi Bleeding: Rohman AzzamgebyarayuNo ratings yet
- Cirrhosis Hepatic: DinadewisliDocument47 pagesCirrhosis Hepatic: DinadewisliwilmaNo ratings yet
- Chronic Liver DiseaseDocument7 pagesChronic Liver DiseaseOnly MrcpNo ratings yet
- MANAGING ACUTE GI BLEEDINGDocument35 pagesMANAGING ACUTE GI BLEEDINGharsani auroraNo ratings yet
- GI Bleeding Team Work - 2nd EditionDocument9 pagesGI Bleeding Team Work - 2nd EditionUsman Ali AkbarNo ratings yet
- Management of Upper Gastrointestinal BleedingDocument62 pagesManagement of Upper Gastrointestinal BleedingAgustinus FatollaNo ratings yet
- GI BLEEDING PresentationDocument47 pagesGI BLEEDING PresentationEsere ObodoNo ratings yet
- Litiasis VesicularDocument26 pagesLitiasis VesicularEULER FARADAY ALTAMIRANO FARFANNo ratings yet
- Pancreatitis & Pseudocyst in ChildrenDocument56 pagesPancreatitis & Pseudocyst in ChildrendrkiranmNo ratings yet
- ABDOMINAL DISTENSION CAUSES AND MANAGEMENTDocument36 pagesABDOMINAL DISTENSION CAUSES AND MANAGEMENTANENA RHODANo ratings yet
- Approaches to Evaluating a Patient with AscitesDocument7 pagesApproaches to Evaluating a Patient with AscitesRavi KumarNo ratings yet
- History Taking for Gallstones (CholelithiasisDocument6 pagesHistory Taking for Gallstones (CholelithiasisToria053No ratings yet
- Perdarahan Saluran Cerna Atas Dan BawahDocument24 pagesPerdarahan Saluran Cerna Atas Dan BawahTia AriantiNo ratings yet
- Doctor's Visit Takes A Funny TurnDocument106 pagesDoctor's Visit Takes A Funny TurnaahadNo ratings yet
- Hematochezia Causes and ManagementDocument33 pagesHematochezia Causes and ManagementMink M SarjanaNo ratings yet
- SURG Abomen CLINICSDocument5 pagesSURG Abomen CLINICSMeg AmoonNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Alcoholism and HepatitisDocument15 pagesAlcoholism and HepatitisTom MallinsonNo ratings yet
- Acute GI BleedingDocument35 pagesAcute GI BleedingGalih GimastiarNo ratings yet
- Specific Diseases: Special PathologyDocument19 pagesSpecific Diseases: Special Pathologyhumag143No ratings yet
- Approach To A Case of HematuriaDocument23 pagesApproach To A Case of HematuriaSunil KumarNo ratings yet
- Approach To A Case of HematuriaDocument23 pagesApproach To A Case of HematuriaSunil KumarNo ratings yet
- Upper Gastrointestinal Bleeding: Fajar Yuwanto SMF Penyakit Dalam RSUD Abdul MoeloekDocument44 pagesUpper Gastrointestinal Bleeding: Fajar Yuwanto SMF Penyakit Dalam RSUD Abdul MoeloekIhsanul RidhoNo ratings yet
- Distal To Ligament of Treitz: CausesDocument8 pagesDistal To Ligament of Treitz: CausesKiara GovenderNo ratings yet
- MBChB Year 5 Lower GI Surgery Core CurriculumDocument3 pagesMBChB Year 5 Lower GI Surgery Core CurriculumJason HarryNo ratings yet
- Perdarahan Saluran Cerna Bagian BawahDocument33 pagesPerdarahan Saluran Cerna Bagian BawahGiyani LiberthiNo ratings yet
- 3.2 Hematemesis LsyDocument23 pages3.2 Hematemesis Lsymirabel IvanaliNo ratings yet
- Liver CirrhosisDocument3 pagesLiver CirrhosisYalin AbouhassiraNo ratings yet
- MalabsorpsiDocument49 pagesMalabsorpsiSyarifah FauziahNo ratings yet
- Dysphagia in ElderyDocument16 pagesDysphagia in ElderySyarifah FauziahNo ratings yet
- Dr. Masitha Dewi S, SP.M Sub Bag. Vitreoretina Ilmu P. Mata: FK - Usu/Rsup H.Adam Malik MedanDocument94 pagesDr. Masitha Dewi S, SP.M Sub Bag. Vitreoretina Ilmu P. Mata: FK - Usu/Rsup H.Adam Malik MedanSyarifah FauziahNo ratings yet
- Introduction & VomitingDocument47 pagesIntroduction & VomitingSyarifah FauziahNo ratings yet
- Hematemesis, Melena, HematoscheziaDocument48 pagesHematemesis, Melena, HematoscheziaSyarifah FauziahNo ratings yet
- K12 - Genetic CounselingDocument36 pagesK12 - Genetic CounselingSyarifah FauziahNo ratings yet
- Diarrhoea: Atan Baas SinuhajiDocument45 pagesDiarrhoea: Atan Baas SinuhajiMeirani RizdaputriNo ratings yet
- Physiology of Hearing and Balance: Departemen Fisiologi FK UsuDocument46 pagesPhysiology of Hearing and Balance: Departemen Fisiologi FK UsuSyarifah FauziahNo ratings yet
- ECG Changes in Diabetes MellitusDocument8 pagesECG Changes in Diabetes MellitusSyarifah FauziahNo ratings yet
- (K24) Acute & Chronic LaryngitisDocument47 pages(K24) Acute & Chronic LaryngitisSyarifah Fauziah100% (3)
- Atan Baas Sinuhaji Department of Childhood, School of Medicine, University of North Sumatera MedanDocument8 pagesAtan Baas Sinuhaji Department of Childhood, School of Medicine, University of North Sumatera MedanSyarifah FauziahNo ratings yet
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiNo ratings yet
- Refraction: Dr. Bobby R.E Sitepu, SP.M Departemen Ilmu Kesehatan Mata FK UsuDocument103 pagesRefraction: Dr. Bobby R.E Sitepu, SP.M Departemen Ilmu Kesehatan Mata FK UsuSyarifah FauziahNo ratings yet
- (K14) - Contact LensesDocument33 pages(K14) - Contact LensesSyarifah FauziahNo ratings yet
- GIS2 - K7 - Body Fluid BalanceDocument33 pagesGIS2 - K7 - Body Fluid BalanceSyarifah FauziahNo ratings yet
- Atan Baas Sinuhaji Department of Childhood, School of Medicine, University of North Sumatera MedanDocument19 pagesAtan Baas Sinuhaji Department of Childhood, School of Medicine, University of North Sumatera MedanMilla PavicaNo ratings yet
- K - 33 Abdominal Distention of Masses (Ilmu Kesehatan Anak)Document20 pagesK - 33 Abdominal Distention of Masses (Ilmu Kesehatan Anak)Wahyu Alamsyah DasopangNo ratings yet
- GIS2 - K2 - ConstipationDocument15 pagesGIS2 - K2 - ConstipationSyarifah FauziahNo ratings yet
- Icterus or Jaundice: Department of Childhealth School of Medicine, University of Sumatera Utara MedanDocument39 pagesIcterus or Jaundice: Department of Childhealth School of Medicine, University of Sumatera Utara MedanSyarifah FauziahNo ratings yet
- Intestinal ParasiteDocument51 pagesIntestinal ParasitefeonajaparNo ratings yet
- K - 33 Abdominal Distention of Masses (Ilmu Kesehatan Anak)Document20 pagesK - 33 Abdominal Distention of Masses (Ilmu Kesehatan Anak)Wahyu Alamsyah DasopangNo ratings yet
- GIS2 - K2 - ConstipationDocument15 pagesGIS2 - K2 - ConstipationSyarifah FauziahNo ratings yet
- Viral Infections in Pregnant Women: Risks and PreventionDocument46 pagesViral Infections in Pregnant Women: Risks and PreventionSyarifah FauziahNo ratings yet
- Nutrition in Childhood (Gizi)Document30 pagesNutrition in Childhood (Gizi)Rivhan FauzanNo ratings yet
- Hipertensi Dalam KehamilanDocument47 pagesHipertensi Dalam KehamilanTommy NainggolanNo ratings yet
- Nursing Care Plans for Respiratory and Circulatory IssuesDocument5 pagesNursing Care Plans for Respiratory and Circulatory IssuesApryll Kristin Villaluna ZafeNo ratings yet
- Petroleum Gases, Liquefied Petroleum Gas: IdentificationDocument4 pagesPetroleum Gases, Liquefied Petroleum Gas: IdentificationdigecaNo ratings yet
- Grain Legumes/Pulses Introduction and ImportanceDocument5 pagesGrain Legumes/Pulses Introduction and ImportancesumandhakalNo ratings yet
- SIP Physical SCiDocument8 pagesSIP Physical SCiShane Catherine BesaresNo ratings yet
- Rock Solid Immunity, Naturally - by Rajeev Agarwal R3Document5 pagesRock Solid Immunity, Naturally - by Rajeev Agarwal R3Rajeev B AgarwalNo ratings yet
- 2020 Corportate Sustainability ReportDocument22 pages2020 Corportate Sustainability ReportMohamed KannouNo ratings yet
- Solution Focused TherapyDocument8 pagesSolution Focused Therapyrimpa29No ratings yet
- Leopold Maneuvers Nursing ProcedureDocument3 pagesLeopold Maneuvers Nursing ProcedureDiane grace SorianoNo ratings yet
- Fermentation - How Antibiotics Are Produced by Fermentation TechnologyDocument12 pagesFermentation - How Antibiotics Are Produced by Fermentation TechnologyArfia Chowdhury Arifa88% (57)
- List of Beed Researchers 2 Semester SY 2020-2021 Beed-ADocument5 pagesList of Beed Researchers 2 Semester SY 2020-2021 Beed-AAndamin MalaNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet
- Meat Inspection Certificate For Export of Pork/Pork Products To MalaysiaDocument2 pagesMeat Inspection Certificate For Export of Pork/Pork Products To MalaysiaLingSiewyingNo ratings yet
- SpitzDocument30 pagesSpitzprabhatNo ratings yet
- Asq 3 42 MDocument8 pagesAsq 3 42 MMohammed AlsuwaidiNo ratings yet
- Breaking The Silence - Art TherapyDocument43 pagesBreaking The Silence - Art TherapyAdriana100% (1)
- Guided Reflection 2Document4 pagesGuided Reflection 2Summer SeedsNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet
- Midwifery LedDocument15 pagesMidwifery LedRizka Dita Hidayati100% (1)
- Multi-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseDocument28 pagesMulti-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseSobek1789No ratings yet
- Health Information Technology-HISMLSDocument1 pageHealth Information Technology-HISMLSJanela Escalante TaboraNo ratings yet
- Lec 4 Principles of Health Financing PDFDocument6 pagesLec 4 Principles of Health Financing PDFRem Alfelor100% (1)
- Managing Painful Diabetic NeuropathyDocument26 pagesManaging Painful Diabetic NeuropathyAthalia TalawayNo ratings yet
- IELTS-Style Speaking Test Questions and Answers SportDocument4 pagesIELTS-Style Speaking Test Questions and Answers SportĐại Học Ôn ThiNo ratings yet
- List of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atDocument2 pagesList of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atAdegokeNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- Canine-Assisted Occupational Therapy For Children On The Autism Spectrum: Parents' PerspectivesDocument10 pagesCanine-Assisted Occupational Therapy For Children On The Autism Spectrum: Parents' PerspectivesDaniele PendezaNo ratings yet
- CUI Texto Examen Multimedia Nivel 6 Curso BasicoDocument2 pagesCUI Texto Examen Multimedia Nivel 6 Curso BasicobertoniramiroNo ratings yet
- MSDS for Feldspar PowderDocument7 pagesMSDS for Feldspar PowderRıdvan SürmeliNo ratings yet
- Project ProposalDocument16 pagesProject ProposalMashaal FasihNo ratings yet