You might also like
- Neurodegenerative DiseasesDocument32 pagesNeurodegenerative DiseasesApurba Sarker Apu100% (1)
- 7 - Drugs Used in ParkinsonDocument47 pages7 - Drugs Used in ParkinsonSara AbbasNo ratings yet
- Antiparkinsons DrugsDocument19 pagesAntiparkinsons Drugs39 Nayan BhagatNo ratings yet
- ParkinsonismDocument18 pagesParkinsonismShivsharanNo ratings yet
- Antiparkinsonismdrugsbydr 181226084221Document70 pagesAntiparkinsonismdrugsbydr 181226084221Analiza Kitongan LantayanNo ratings yet
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsDocument57 pagesDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaNo ratings yet
- 4 AntipsychoticDocument109 pages4 AntipsychoticMtw Wond100% (1)
- NeuropharmacologyDocument30 pagesNeuropharmacologytracy_lau_8No ratings yet
- Aashish Parihar Lecturer College of Nursing AIIMS, JodhpurDocument101 pagesAashish Parihar Lecturer College of Nursing AIIMS, JodhpurHardeep KaurNo ratings yet
- Parkinson's DiseaseDocument65 pagesParkinson's DiseaseGerald Resubal OriñaNo ratings yet
- 1CNS IntroductionDocument32 pages1CNS Introductionyonasashagrie34No ratings yet
- Antidepressant and AntimanicDocument60 pagesAntidepressant and Antimanictbuyinza21apNo ratings yet
- Drugs For Parkinson's DiseaseDocument43 pagesDrugs For Parkinson's DiseasesabaNo ratings yet
- Parkinsonism FinalDocument54 pagesParkinsonism FinalvijayNo ratings yet
- Parkinson Disease SlidesDocument21 pagesParkinson Disease Slidessarah morley100% (2)
- Parkinson's DiseaseDocument24 pagesParkinson's Diseasejanemwanza003No ratings yet
- Psychotropic DrugsDocument81 pagesPsychotropic DrugsJoan100% (2)
- Pharmacology of Drugs in Extrapyramidal Disorders: Prof - Aznan Lelo, DR, PHD, SPFK & DR Datten Bangun, MSC, SPFKDocument42 pagesPharmacology of Drugs in Extrapyramidal Disorders: Prof - Aznan Lelo, DR, PHD, SPFK & DR Datten Bangun, MSC, SPFKWinson ChitraNo ratings yet
- Drugs Used in Mental IllnessDocument60 pagesDrugs Used in Mental IllnessDixa MeNo ratings yet
- Antiparkinson Pharma 2020Document26 pagesAntiparkinson Pharma 2020Ida Bagus Putu SwabawaNo ratings yet
- Anti ParkinsonDocument18 pagesAnti ParkinsonRitika DasNo ratings yet
- Block I Posting, Pharmacology Lectures: Antiparkisonian DrugsDocument41 pagesBlock I Posting, Pharmacology Lectures: Antiparkisonian DrugsOdiete EfeNo ratings yet
- Drug Therapy of ParkinsonismDocument28 pagesDrug Therapy of ParkinsonismZobayer AhmedNo ratings yet
- Block I Posting, Pharmacology Lectures: Dr. Aduragbenro AdedapoDocument47 pagesBlock I Posting, Pharmacology Lectures: Dr. Aduragbenro AdedapoOdiete EfeNo ratings yet
- 3.3.4.4 DRUG in PSYCHIATRIC DISORDERDocument31 pages3.3.4.4 DRUG in PSYCHIATRIC DISORDERyunielsyaNo ratings yet
- Psychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditDocument99 pagesPsychopharmacology - Dr. Citra Ayu Aprilia, M.kes - Rabu 19 Oktober 2022 - 07.00 - 08.50 - EditCITRA AYU APRILIANo ratings yet
- Right-Hand Tremor at Rest, WhichDocument47 pagesRight-Hand Tremor at Rest, WhichsyarintaadeninaNo ratings yet
- Cns Trans & Drug DetoxificationDocument57 pagesCns Trans & Drug DetoxificationAlvin LaurenceNo ratings yet
- Parkinson's DiseaseDocument37 pagesParkinson's DiseaseAhmed OsamaNo ratings yet
- Pharmacology of Drugs Acting On Central Nervous System 1st (Mam) PDFDocument47 pagesPharmacology of Drugs Acting On Central Nervous System 1st (Mam) PDFRahul palsNo ratings yet
- Bms166 Slide Antipsychotic AntidepressantDocument52 pagesBms166 Slide Antipsychotic AntidepressantErmanto D'PhytoxzNo ratings yet
- Pharma - Anti Parkinsons Dra JusayanDocument105 pagesPharma - Anti Parkinsons Dra JusayanNikko AgcaoiliNo ratings yet
- CNS NeurotransmitterDocument67 pagesCNS NeurotransmitterGreenNo ratings yet
- AntidepressantsDocument38 pagesAntidepressantsjabari.baraNo ratings yet
- AntipsychoticsDocument47 pagesAntipsychoticsammar_ahmed_19No ratings yet
- Central Nervous System Agents: Carmencita R. Pacis PHD, ManDocument52 pagesCentral Nervous System Agents: Carmencita R. Pacis PHD, ManTWINNY JOSSANNE CHEERISHANE MINIONNo ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- Lecture 27 - 3rd Asessment - CNS IntroductionDocument31 pagesLecture 27 - 3rd Asessment - CNS Introductionapi-3703352100% (1)
- Lect 3A - Other Drugs Act On The CNS - 29 Sept 2021Document49 pagesLect 3A - Other Drugs Act On The CNS - 29 Sept 2021Garry SoloanNo ratings yet
- Parkinson'sDocument42 pagesParkinson'sjabari.baraNo ratings yet
- Neuroleptics (Antipsychotics) : DR S. A Jayaratne Senior Lecturer Dept of PharamacologyDocument21 pagesNeuroleptics (Antipsychotics) : DR S. A Jayaratne Senior Lecturer Dept of PharamacologysivaNo ratings yet
- Introduction To Cns PharmacologyDocument66 pagesIntroduction To Cns PharmacologyYazan Emad Salem100% (1)
- Movement Abnormalities Associated With Psychopharmacologic AgentsDocument31 pagesMovement Abnormalities Associated With Psychopharmacologic AgentsAbelNo ratings yet
- Second Gen AtipsychoticDocument34 pagesSecond Gen Atipsychoticemamma hashirNo ratings yet
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanDocument51 pagesPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganNo ratings yet
- Sedation & Neuromuscular Blockade: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument58 pagesSedation & Neuromuscular Blockade: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaZEMENAY TRUNEHNo ratings yet
- 5-Drugs Used in Parkinsonism Summary and QuestionsDocument7 pages5-Drugs Used in Parkinsonism Summary and QuestionsmugtabaNo ratings yet
- Neurotransmitters and NeuromodulatorsDocument38 pagesNeurotransmitters and NeuromodulatorsStanleyNo ratings yet
- Drugs That Cause and Drugs That Alleviate Parkinsonism: BY Prof. Mbah A.UDocument24 pagesDrugs That Cause and Drugs That Alleviate Parkinsonism: BY Prof. Mbah A.UtemitopeNo ratings yet
- Anti ParkinsonDocument29 pagesAnti Parkinsonking_gold100% (1)
- Module II 2 - ParkinsonsDocument39 pagesModule II 2 - Parkinsonsaysha jasimNo ratings yet
- Overview CNS Chemical TransmissionDocument75 pagesOverview CNS Chemical TransmissionsaivasyaNo ratings yet
- Cns Stimulants...Document24 pagesCns Stimulants...Ramya RNo ratings yet
- Antiparkinsonian DrugsDocument35 pagesAntiparkinsonian DrugsvimalaNo ratings yet
- K10 (A1) - 2015pharmacotherapy For ParkinsonDocument41 pagesK10 (A1) - 2015pharmacotherapy For Parkinsonali100% (1)
- Drug Study AntipsychoticDocument7 pagesDrug Study AntipsychoticLouela de Asas100% (2)
- Obat Antiparkinson 2010Document18 pagesObat Antiparkinson 2010ludoy03No ratings yet
- AntiepilepticsDocument25 pagesAntiepilepticsMurali Krishna Kumar MuthyalaNo ratings yet
- Pharmacological Treatment: Antipsychotics: Mechanism of ActionDocument7 pagesPharmacological Treatment: Antipsychotics: Mechanism of Actionvarsha thakurNo ratings yet
- CV. LathatnamexayDocument1 pageCV. LathatnamexayLathtanamexay SOULIYANONNo ratings yet
- Aniline Derivatives (Drugs)Document4 pagesAniline Derivatives (Drugs)Arljayn Cuachon100% (1)
- RuscogeninDocument6 pagesRuscogeninNawaz SfNo ratings yet
- Drug Abuse: Short-Term EffectsDocument2 pagesDrug Abuse: Short-Term EffectsYeonjin ChoiNo ratings yet
- Matching: KEY Unit 1: Pharmaceutical Sciences I. VocabularyDocument22 pagesMatching: KEY Unit 1: Pharmaceutical Sciences I. VocabularyHồ Như Tân100% (1)
- Oss Oeric Psilocybin Magic Mushroom Growers GuideDocument42 pagesOss Oeric Psilocybin Magic Mushroom Growers Guidesebasdixit100% (4)
- Top 500 2016Document12 pagesTop 500 2016RicardoHerediaNo ratings yet
- Pharmacy Management Lec 1 PDFDocument21 pagesPharmacy Management Lec 1 PDFMalek MohamedNo ratings yet
- Topical Drugs in DentistryDocument6 pagesTopical Drugs in DentistryIyad Abou-RabiiNo ratings yet
- Challenges To Implementation of The Pharmaceutical Care Practice in Davao City.Document11 pagesChallenges To Implementation of The Pharmaceutical Care Practice in Davao City.JessieLynMolinaNo ratings yet
- PR Tianma Perlieremimi Impactra Final-100220Document10 pagesPR Tianma Perlieremimi Impactra Final-100220jerryNo ratings yet
- Abidec DropsDocument6 pagesAbidec DropsRouag AbdelkarimNo ratings yet
- Disintegration TestDocument13 pagesDisintegration TestVesh Chaurasiya100% (1)
- FDA PPT of Definitions Emulsion SuspensionDocument15 pagesFDA PPT of Definitions Emulsion SuspensionvijayrnjnNo ratings yet
- Sanofi-Aventis Presentation On FlagylDocument24 pagesSanofi-Aventis Presentation On FlagylNasir Ali100% (3)
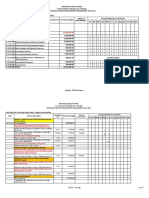
- 2021 PPMP - Projects-HSFESP-FINALDocument20 pages2021 PPMP - Projects-HSFESP-FINALKimscey Yvan DZ SulitNo ratings yet
- Drug StudyDocument9 pagesDrug StudyRaymond Reyes GuanzonNo ratings yet
- CLEVIDIPINE CleviprexDocument17 pagesCLEVIDIPINE Cleviprextpwarren23No ratings yet
- ###Tutorial Work 217 Questions and Answers Mcqs PDFDocument32 pages###Tutorial Work 217 Questions and Answers Mcqs PDFDave DMNo ratings yet
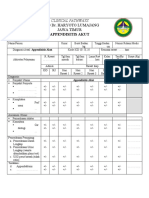
- Clinical Pathway SMF BEDAH 2021Document39 pagesClinical Pathway SMF BEDAH 2021ikesesaria100% (1)
- Project Charter: Project Name: Smart Medical Box Group MembersDocument2 pagesProject Charter: Project Name: Smart Medical Box Group MembersMr ABDULLAHNo ratings yet
- The High Cost of Prescriptions - JAMADocument26 pagesThe High Cost of Prescriptions - JAMAamp0201No ratings yet
- Ranitidine Drug StudyDocument2 pagesRanitidine Drug StudyMarvie Cadena100% (3)
- Basic Infection Control Prevention Plan 2011Document21 pagesBasic Infection Control Prevention Plan 2011adadanNo ratings yet
- Stock 29.04.23Document5 pagesStock 29.04.23Kasi HumasNo ratings yet
- The Truth About CBDDocument34 pagesThe Truth About CBDapi-458412381No ratings yet
- Laporan Stoc ObatDocument34 pagesLaporan Stoc ObatAyouItuYustirahayuNo ratings yet
- Sun Pharma Ind Annuals Report (Final) 707Document151 pagesSun Pharma Ind Annuals Report (Final) 707ÄbhíñävJäíñNo ratings yet
- Bagian Farmasi 9 Nov 2020Document8 pagesBagian Farmasi 9 Nov 2020AbePrasetyaNo ratings yet
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDocument39 pagesLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuNo ratings yet