You might also like
- Medical Auditing Training: CPMA®: Practical Application WorkbookDocument22 pagesMedical Auditing Training: CPMA®: Practical Application WorkbookAnthony El HageNo ratings yet
- Bone Augmentation by Anatomical RegionDocument552 pagesBone Augmentation by Anatomical RegionIon Baltaga100% (5)
- Ineffective Airway Clearance Related To SinusitisDocument3 pagesIneffective Airway Clearance Related To SinusitisBarbara Detaro71% (7)
- SinusitisDocument30 pagesSinusitisAbdiqani MahdiNo ratings yet
- Sinus Problems Stop!: The Complete Guide on Sinus Infection, Sinusitis Symptoms, Sinusitis Treatment, & Secrets to Natural Sinus Relief without Harsh DrugsFrom EverandSinus Problems Stop!: The Complete Guide on Sinus Infection, Sinusitis Symptoms, Sinusitis Treatment, & Secrets to Natural Sinus Relief without Harsh DrugsNo ratings yet
- Kewenangan Klinis Spesialis THTDocument8 pagesKewenangan Klinis Spesialis THTANONIM100% (1)
- Lesson 5 - Disaster ManagementDocument40 pagesLesson 5 - Disaster ManagementHampson MalekanoNo ratings yet
- NCM 113 Upper Respiratory DiseaseDocument68 pagesNCM 113 Upper Respiratory DiseaseJerah Aceron SatorreNo ratings yet
- Ent Explain Why and Short Notes by Shuvro DaDocument37 pagesEnt Explain Why and Short Notes by Shuvro DaSumanNo ratings yet
- EPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Document34 pagesEPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Julliza Joy PandiNo ratings yet
- Acute SinusitisDocument11 pagesAcute Sinusitisعبدالله فائز غلامNo ratings yet
- SINUSITIS-WPS OfficeDocument3 pagesSINUSITIS-WPS OfficeDolly DollyNo ratings yet
- B.ing PaperDocument15 pagesB.ing PaperAriph BudiboyNo ratings yet
- University of Diyala: College of Medicine The First StageDocument7 pagesUniversity of Diyala: College of Medicine The First StageHunter X HunterNo ratings yet
- Rhinology: The Affiliated Hospital of Ningxia Medical College TEL:13895082698Document19 pagesRhinology: The Affiliated Hospital of Ningxia Medical College TEL:13895082698ArvindhanNo ratings yet
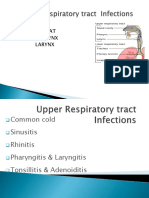
- Parts: Nose Throat Pharynx LarynxDocument47 pagesParts: Nose Throat Pharynx LarynxRANJIT GOGOINo ratings yet
- SinusitisDocument23 pagesSinusitisMumin Alamin AllaminNo ratings yet
- What and Where Are The Sinuses?Document10 pagesWhat and Where Are The Sinuses?jercx_trigaNo ratings yet
- Treatment of Maxillary SinusitisDocument15 pagesTreatment of Maxillary SinusitisRabina PantaNo ratings yet
- Maxillary SinusitisDocument28 pagesMaxillary SinusitisSumaNo ratings yet
- Maxillary SinusDocument43 pagesMaxillary SinusAli FalihNo ratings yet
- Disorder of NoseDocument31 pagesDisorder of NoseSumit YadavNo ratings yet
- Deviated Nasal SeptumDocument15 pagesDeviated Nasal SeptumSrinivas Sukhavasi50% (2)
- Upper Resp. Tract InfectionDocument45 pagesUpper Resp. Tract InfectionFarwaNo ratings yet
- ADENOIDITISDocument4 pagesADENOIDITISMartha AsikoNo ratings yet
- What Is Sinusitis?Document4 pagesWhat Is Sinusitis?Srikamal SinganamalaNo ratings yet
- Symptoms of Nasal PolypsDocument5 pagesSymptoms of Nasal Polypspratik hamalNo ratings yet
- Disorders of EarDocument17 pagesDisorders of EarharpreetNo ratings yet
- Sinusitis: Causes, Incidence, and Risk FactorsDocument5 pagesSinusitis: Causes, Incidence, and Risk FactorsDyane VatriciaNo ratings yet
- What Are Sinuses?Document3 pagesWhat Are Sinuses?Valentine WijayaNo ratings yet
- Bharat Singh Banshiwal: Asst. Professor M.Sc. Nursing (Med.-Surg. Nursing) Jiet College of Nursing, JodhpurDocument11 pagesBharat Singh Banshiwal: Asst. Professor M.Sc. Nursing (Med.-Surg. Nursing) Jiet College of Nursing, JodhpurBharat Singh BanshiwalNo ratings yet
- Upper Airway InfectionDocument47 pagesUpper Airway Infectionjm_john0% (1)
- Basog - ReportTonsillitis and EpistaxisDocument4 pagesBasog - ReportTonsillitis and EpistaxisclaribelleNo ratings yet
- Upper Respiratory Tract InfectionDocument45 pagesUpper Respiratory Tract InfectionNatasha Abdulla100% (2)
- Importance of Indicators of Nitroxidergic System in Improving The Treatment of Acute and Chronic Purulent SinusitisDocument4 pagesImportance of Indicators of Nitroxidergic System in Improving The Treatment of Acute and Chronic Purulent SinusitisCentral Asian StudiesNo ratings yet
- MED SURG OUTLINE Chapter 14 Care of Patients With Disorders of Upper Respiratory SystemDocument6 pagesMED SURG OUTLINE Chapter 14 Care of Patients With Disorders of Upper Respiratory SystemMichaela LemanNo ratings yet
- 1.0 Upper Airway InfectionsDocument45 pages1.0 Upper Airway InfectionsMariahNo ratings yet
- Chapter10 INFLAMMATORY CONDITION OF NOSE & PNSDocument38 pagesChapter10 INFLAMMATORY CONDITION OF NOSE & PNSSULDAANUL CAASHIQIINNo ratings yet
- No 13Document2 pagesNo 13Bang mantoNo ratings yet
- SinusitisDocument3 pagesSinusitisRohan SuryagandhNo ratings yet
- IVRSDocument61 pagesIVRSAndrew ChinchillaNo ratings yet
- 2 RHINOLOGY SinusDocument87 pages2 RHINOLOGY SinusWai Kwong ChiuNo ratings yet
- Sinusitis in ChildDocument14 pagesSinusitis in ChildKin molikaNo ratings yet
- Foreign Body in The NoseDocument32 pagesForeign Body in The NoseLady350zNo ratings yet
- Penyebab Otalgia 2010Document11 pagesPenyebab Otalgia 2010siska tiaraNo ratings yet
- Penyebab Otalgia 2010 PDFDocument11 pagesPenyebab Otalgia 2010 PDFnotpentingNo ratings yet
- Jordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryDocument11 pagesJordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryJordan Abosama MamalumpongNo ratings yet
- Nasal PolypsDocument1 pageNasal PolypsFiljordan LulupoyNo ratings yet
- Q Oral IU 2023Document4 pagesQ Oral IU 2023Kin molikaNo ratings yet
- Nursing Management of Children With Respiratory System DysfunctionsDocument27 pagesNursing Management of Children With Respiratory System DysfunctionsDody ZainNo ratings yet
- Sinusitis 2000Document7 pagesSinusitis 2000GenaroMallquiNo ratings yet
- Acute and Chronic Otitis MediaDocument32 pagesAcute and Chronic Otitis MediaAndrew KaumbaNo ratings yet
- Middle Ear Infections: Buy The BookDocument6 pagesMiddle Ear Infections: Buy The BookAndi Astrid AgustinaNo ratings yet
- Otitis MediaDocument55 pagesOtitis MediaJollyann SedaNo ratings yet
- Acuite Otitis Media Final PresentationDocument26 pagesAcuite Otitis Media Final Presentationmohamedkallon1996No ratings yet
- SinusitisDocument6 pagesSinusitisRae Marie AquinoNo ratings yet
- Respiratory Disorder: BY Hidayat Khan MSN, MPH, BSN, & Chpe, Ip&C, Rn. DPHNDocument89 pagesRespiratory Disorder: BY Hidayat Khan MSN, MPH, BSN, & Chpe, Ip&C, Rn. DPHNSyed MaazNo ratings yet
- Nasal Obstruction: Nitha K 2nd Year MSC NursingDocument65 pagesNasal Obstruction: Nitha K 2nd Year MSC NursingNITHA KNo ratings yet
- Nasal PolypsDocument4 pagesNasal PolypsGaby Fitria BahriNo ratings yet
- Sinus Barotrauma: Anatomy of The SinusesDocument5 pagesSinus Barotrauma: Anatomy of The SinusesanyumiyyahNo ratings yet
- Krishna Reddy Inflammations of NasopharynxDocument18 pagesKrishna Reddy Inflammations of NasopharynxSiva ramaNo ratings yet
- Otits MediaDocument68 pagesOtits MediaSaidi EdwardNo ratings yet
- Acute SinusitisDocument7 pagesAcute SinusitisNader SmadiNo ratings yet
- Hypertension B.MDocument37 pagesHypertension B.MBwalya MunjiliNo ratings yet
- Mastoiditis - B.MDocument25 pagesMastoiditis - B.MBwalya MunjiliNo ratings yet
- Otn Sutures and Equipmaent - B.MDocument52 pagesOtn Sutures and Equipmaent - B.MBwalya MunjiliNo ratings yet
- Surgical Incisions Power Point B - MDocument21 pagesSurgical Incisions Power Point B - MBwalya MunjiliNo ratings yet
- Preparation of Ot B.MDocument47 pagesPreparation of Ot B.MBwalya MunjiliNo ratings yet
- Positions Used in Surgery B.MDocument29 pagesPositions Used in Surgery B.MBwalya MunjiliNo ratings yet
- Introduction To Theatre Nursing B.MDocument46 pagesIntroduction To Theatre Nursing B.MBwalya MunjiliNo ratings yet
- Garib (2010) - Alveolar Bone Morphology Under The Perspective of The Computed Tomography. Defining The Biological Limits of Tooth Movement PDFDocument15 pagesGarib (2010) - Alveolar Bone Morphology Under The Perspective of The Computed Tomography. Defining The Biological Limits of Tooth Movement PDFIsmaelLouGomezNo ratings yet
- Entellus Medical Presentation August 2016 - Canaccord - LONGDocument28 pagesEntellus Medical Presentation August 2016 - Canaccord - LONGmedtechyNo ratings yet
- Pediatric Sinusitis and Sinus SurgeryDocument293 pagesPediatric Sinusitis and Sinus SurgerywillyoueverlovemenkNo ratings yet
- Maxillary Sinus Augmentation: Tarun Kumar A.B, Ullas AnandDocument13 pagesMaxillary Sinus Augmentation: Tarun Kumar A.B, Ullas AnandMazenShbeebNo ratings yet
- Maxillary Sinus Diseases: Click To Edit Master Title StyleDocument75 pagesMaxillary Sinus Diseases: Click To Edit Master Title StylePooja JaiswalNo ratings yet
- Knottenbelt and Pascoe's Color Atlas of Diseases and Disorders of The Horse-Saunders (VetBooks - Ir)Document538 pagesKnottenbelt and Pascoe's Color Atlas of Diseases and Disorders of The Horse-Saunders (VetBooks - Ir)Roger Fernando Abril DiazNo ratings yet
- Cranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)Document51 pagesCranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)abo kooNo ratings yet
- Nasal Stents Are They Really Useful ?Document9 pagesNasal Stents Are They Really Useful ?Dr. T. BalasubramanianNo ratings yet
- Inverted Papilloma Nose and Its ManagementDocument20 pagesInverted Papilloma Nose and Its ManagementDr. T. Balasubramanian100% (3)
- Local Anesthesia in Pediatric Dentistry Lecture Students 2009 MDocument88 pagesLocal Anesthesia in Pediatric Dentistry Lecture Students 2009 MIoana DănilăNo ratings yet
- The Skeleton: Chapter 7 - Part ADocument7 pagesThe Skeleton: Chapter 7 - Part AJonathan HigginbothamNo ratings yet
- Dental and Craniomaxillofacial Implant SurgeryDocument35 pagesDental and Craniomaxillofacial Implant SurgeryJean Carlos Barbosa FerreiraNo ratings yet
- Core Radiology - Head & Neck ImagingDocument106 pagesCore Radiology - Head & Neck ImagingefqsdfqsNo ratings yet
- Oral Surgery, Oral Diagnosis, Roentgenology: B. A Radiolucent Halo Surrounding The Root of The FractureDocument49 pagesOral Surgery, Oral Diagnosis, Roentgenology: B. A Radiolucent Halo Surrounding The Root of The FractureRC Dome100% (1)
- Maxillary Sinus in Health and DiseaseDocument36 pagesMaxillary Sinus in Health and Diseasedaw022No ratings yet
- Principles of Designing Mucoperiosteal FlapsDocument70 pagesPrinciples of Designing Mucoperiosteal FlapsStephen KinyanjuiNo ratings yet
- Maxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document24 pagesMaxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNo ratings yet
- Traslate Bab 8 TopazianDocument87 pagesTraslate Bab 8 TopazianAnonymous bLf4glCRffNo ratings yet
- WEEKLY Study Plan DentistryDocument14 pagesWEEKLY Study Plan DentistryWarisha AmirNo ratings yet
- Choanal Atresia PDFDocument8 pagesChoanal Atresia PDFMonna Medani LysabellaNo ratings yet
- Anatomy of Nasal CavityDocument37 pagesAnatomy of Nasal Cavityjony lever100% (1)
- Maxillary NerveDocument26 pagesMaxillary NerveHanaMajeedNo ratings yet
- 2 OS To PrintDocument12 pages2 OS To PrintDENTAL REVIEWER ONLY0% (1)
- Treatment of Maxillary SinusitisDocument15 pagesTreatment of Maxillary SinusitisRabina PantaNo ratings yet
- Nasal Cavity and Paranasal Sinuses: Anatomy and FunctionDocument17 pagesNasal Cavity and Paranasal Sinuses: Anatomy and FunctionVictor EnachiNo ratings yet
- Changes in Mucociliary Clearance and Olfaction Following Endoscopic Sinus SurgeryDocument20 pagesChanges in Mucociliary Clearance and Olfaction Following Endoscopic Sinus SurgerygoolnuulNo ratings yet
- Head and Neck Anatomy Study NotesDocument7 pagesHead and Neck Anatomy Study NotesJode GroenewaldtNo ratings yet