You might also like
- PASSMED MRCP MCQs-INFECTIOUS DISEASES CompleteDocument131 pagesPASSMED MRCP MCQs-INFECTIOUS DISEASES CompleteStarlight100% (1)
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- KSA EndodonticsDocument7 pagesKSA EndodonticsHitesh Chopra100% (6)
- Healing Colon Liver and Pancreas Cancer - The Gerson WayDocument18 pagesHealing Colon Liver and Pancreas Cancer - The Gerson Waytzibellaris67% (3)
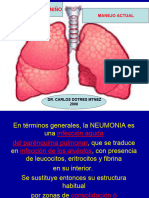
- Med PPT Pneumonia For LectureDocument67 pagesMed PPT Pneumonia For LectureManisanthosh Kumar100% (1)
- Management of Obstetric Emergencies Y5Document80 pagesManagement of Obstetric Emergencies Y5Charles Wilson83% (6)
- ACOG Fecal Incontinence.2019Document14 pagesACOG Fecal Incontinence.2019linaNo ratings yet
- Background: Mandrillari SDocument9 pagesBackground: Mandrillari SDewi ArdianaNo ratings yet
- ToxoplasmosisDocument5 pagesToxoplasmosisValerrie NgenoNo ratings yet
- Free Living Amebae Garcia 667-691Document7 pagesFree Living Amebae Garcia 667-691evelynseaaNo ratings yet
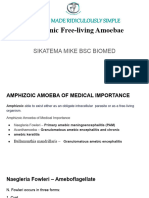
- Pathogenic and Free Living Amoeba Sikatema MikeDocument33 pagesPathogenic and Free Living Amoeba Sikatema MikebrainworxeducationNo ratings yet
- Current Trends in The Management of MalariaDocument41 pagesCurrent Trends in The Management of Malariaghr9cjy5npNo ratings yet
- Meningococcemia: Neisseria Meningitidis - Is An EncapsulatedDocument19 pagesMeningococcemia: Neisseria Meningitidis - Is An EncapsulatedcarolinecayasaNo ratings yet
- BB30052 Scientific Communication: The Pathophysiology ofDocument10 pagesBB30052 Scientific Communication: The Pathophysiology ofCendani LarasNo ratings yet
- Naegleria FowleriDocument14 pagesNaegleria FowleriAya AyaNo ratings yet
- Choosing AntibioticsDocument16 pagesChoosing AntibioticsHenry CollazosNo ratings yet
- Background: Mycobacterium Avium Complex (MAC) Consists of 2Document14 pagesBackground: Mycobacterium Avium Complex (MAC) Consists of 2readyboy89No ratings yet
- 10 5530ijmedph 2016 3 11Document3 pages10 5530ijmedph 2016 3 11wahyu agungNo ratings yet
- Respiratory: Crash Revision Omar K. MRCP IrelandDocument61 pagesRespiratory: Crash Revision Omar K. MRCP IrelandManmeet SNo ratings yet
- International Journal For Parasitology: Samuel Crocodile Wassmer, Georges Emile Raymond GrauDocument8 pagesInternational Journal For Parasitology: Samuel Crocodile Wassmer, Georges Emile Raymond GrauDelvina RahmadaniNo ratings yet
- Cours de MedcineDocument11 pagesCours de MedcineLAYLA AIZANo ratings yet
- ImleDocument225 pagesImleDaniel StepanovNo ratings yet
- Cap, Hap, VapDocument63 pagesCap, Hap, Vapbekbekk cabahugNo ratings yet
- Nocardia, Bordetella, HaemophilusDocument31 pagesNocardia, Bordetella, HaemophilusLourdes Cumagon BasiuangNo ratings yet
- Staphylococcal Toxic Shock Syndrome: M Kare, A DangDocument3 pagesStaphylococcal Toxic Shock Syndrome: M Kare, A DangAnonymous ALlIo2LNo ratings yet
- Micro NotesDocument29 pagesMicro NotesRoberto Christian Cerrud RodríguezNo ratings yet
- Trypanosoma-SppDocument4 pagesTrypanosoma-SppVE NI CENo ratings yet
- Atypical PneumoniaDocument30 pagesAtypical PneumoniachandanNo ratings yet
- Streptococcus SPPDocument52 pagesStreptococcus SPPdrnuaman5No ratings yet
- Cns InfectionsDocument141 pagesCns InfectionsReda AlyNo ratings yet
- Intestinal Protozoa: Entamoeba Histolytica Giardia Lamblia Cryptosporidium ParvumDocument12 pagesIntestinal Protozoa: Entamoeba Histolytica Giardia Lamblia Cryptosporidium Parvumshiner99No ratings yet
- Malaria HODocument45 pagesMalaria HOnitsuhNo ratings yet
- 46-Year-Old Man With Fevers, Chills, and PancytopeniaDocument4 pages46-Year-Old Man With Fevers, Chills, and PancytopeniaDr Manoranjan MNo ratings yet
- Medicine Lec.12 - Protozoal InfectionDocument60 pagesMedicine Lec.12 - Protozoal Infection7fefdfbea1No ratings yet
- Opportunistic Amoebae: Challenges in Prophylaxis and TreatmentDocument11 pagesOpportunistic Amoebae: Challenges in Prophylaxis and TreatmentColette BarrometroNo ratings yet
- Asymptomatic Mycoplasma Infection Causing Acute Demyelinating Encephalomyelitis: Case Report and Review of LiteratureDocument4 pagesAsymptomatic Mycoplasma Infection Causing Acute Demyelinating Encephalomyelitis: Case Report and Review of Literatureluisalfredo_montesNo ratings yet
- (MIKROBIOLOGI) IT 20 - Orthomyxovirus, Paramyxovirus - KHSDocument37 pages(MIKROBIOLOGI) IT 20 - Orthomyxovirus, Paramyxovirus - KHSRessy FelisaNo ratings yet
- Choosing Optimal Antimicrobial TherapiesDocument16 pagesChoosing Optimal Antimicrobial Therapiesqhrn48psvwNo ratings yet
- Other Bacteria With Unusual Growth Requirements PDFDocument102 pagesOther Bacteria With Unusual Growth Requirements PDFNova Amor MahayagNo ratings yet
- Sulphonamides & Co - Trimoxazole BamsDocument46 pagesSulphonamides & Co - Trimoxazole BamsKasturiRangan SrivatsaNo ratings yet
- Group A Streptococcal Infections: PatophysiologyDocument11 pagesGroup A Streptococcal Infections: Patophysiologyrahma perwitasariNo ratings yet
- Pneumonia by Kamran UOSargodhaDocument19 pagesPneumonia by Kamran UOSargodhaZeshan Haider Kazmi100% (3)
- Cns ParasitesDocument74 pagesCns Parasitesahmed12mohamed12hNo ratings yet
- Actue Management of Pneumonia in Adults PatienitDocument8 pagesActue Management of Pneumonia in Adults Patienitxiomara torresNo ratings yet
- (MIKROBIOLOGI) IT 20 - Orthomyxovirus, Paramyxovirus - KHSDocument37 pages(MIKROBIOLOGI) IT 20 - Orthomyxovirus, Paramyxovirus - KHSYUFFANo ratings yet
- Respiratory DiseasesDocument14 pagesRespiratory DiseasesJari JariNo ratings yet
- Journal Pre-Proof: IdcasesDocument8 pagesJournal Pre-Proof: IdcasesDaniel GuevaraNo ratings yet
- Malaria CerebralDocument2 pagesMalaria CerebralDiana Fadhilah SariNo ratings yet
- Control of plumonary-WPS OfficeDocument15 pagesControl of plumonary-WPS OfficeopeoluwaestheraNo ratings yet
- Streptococcus Pneumoniae Voice PresentationDocument21 pagesStreptococcus Pneumoniae Voice Presentationchristopher lopezNo ratings yet
- MOST IMPORATANT ONE LINERS Compiled by Medicinosis Magnus 2Document18 pagesMOST IMPORATANT ONE LINERS Compiled by Medicinosis Magnus 2VAIBHAV SHARMA- 122No ratings yet
- Malaria: What's New in The Management of Malaria?Document22 pagesMalaria: What's New in The Management of Malaria?wiwiNo ratings yet
- Acute Bacterial MeningitiDocument31 pagesAcute Bacterial MeningitiHesbon MomanyiNo ratings yet
- AudioDocument50 pagesAudioshortysdavidNo ratings yet
- Antibiotics IN Maxillofacial Surgery: Presenter: Dr. Venu G.RDocument92 pagesAntibiotics IN Maxillofacial Surgery: Presenter: Dr. Venu G.RkatnevNo ratings yet
- Pubid-848078832 1010 PDFDocument10 pagesPubid-848078832 1010 PDFCocosul Cocosului CocosaruluiNo ratings yet
- MalariaDocument17 pagesMalariaDestri NeliNo ratings yet
- IMMS Viruses. Basics: A-And A-Interferon A-InterferonDocument4 pagesIMMS Viruses. Basics: A-And A-Interferon A-Interferonrosanna_hildersleyNo ratings yet
- Pyogenic and TB Meningitis - FinalDocument65 pagesPyogenic and TB Meningitis - FinalKishor K AdhikariNo ratings yet
- Entamoeba Coli: E. HistolyticaDocument15 pagesEntamoeba Coli: E. HistolyticaDavid Tritono Di BallastrossNo ratings yet
- Neumonías 2008Document62 pagesNeumonías 2008Lucero BautistaNo ratings yet
- Meningitis Pathophysiology PDFDocument59 pagesMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- Cebu Normal University Graduate SchoolDocument42 pagesCebu Normal University Graduate Schoolmaeliszxc kimNo ratings yet
- 151 English-1Document10 pages151 English-1Michael KaiNo ratings yet
- NCM116B PrelimRequirements BermasDocument5 pagesNCM116B PrelimRequirements BermasChristian BenomanNo ratings yet
- Pathology Notes (Class Notes)Document106 pagesPathology Notes (Class Notes)Mustafa Kamal Bangash100% (1)
- Endocrine System: Prepared By: Richer Irish B. EvangelistaDocument29 pagesEndocrine System: Prepared By: Richer Irish B. EvangelistaDherick RaleighNo ratings yet
- 6.1 VpaDocument20 pages6.1 VpahenihandayNo ratings yet
- 2010 Goh Vulnera - EngDocument5 pages2010 Goh Vulnera - EngFernandoCedroNo ratings yet
- Cognitive and PsychologicalDocument23 pagesCognitive and PsychologicalIsabel ValdésNo ratings yet
- 5 Questions DR VryghemDocument1 page5 Questions DR VryghemDr. Jérôme C. VryghemNo ratings yet
- Disseminated Intravascular Coagulation: Date/Time F Focus D Date A Action R ResponseDocument11 pagesDisseminated Intravascular Coagulation: Date/Time F Focus D Date A Action R ResponseMJ LomuntadNo ratings yet
- Towards Improving post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons From A Case Study - Calabrò 2019Document8 pagesTowards Improving post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons From A Case Study - Calabrò 2019Julio JuarezNo ratings yet
- Care For Mechanical VentilationDocument14 pagesCare For Mechanical Ventilationmaeya186135100% (3)
- When Is Parenteral Nutrition Appropriate?: Consensus RecommendationDocument54 pagesWhen Is Parenteral Nutrition Appropriate?: Consensus RecommendationÁlvaro TorresNo ratings yet
- ANTENATAL CARE Translate GooglingDocument26 pagesANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- Open Heart Surgery CaabgDocument6 pagesOpen Heart Surgery CaabgGopi KrishnanNo ratings yet
- Cancer Screening QuestionnaireDocument3 pagesCancer Screening QuestionnaireakashniranjaneNo ratings yet
- Renal Arteries PDFDocument18 pagesRenal Arteries PDFServo LedNo ratings yet
- RH D Immunoglobulin (Anti-D)Document4 pagesRH D Immunoglobulin (Anti-D)Ywagar YwagarNo ratings yet
- Disease of Biliary SystemDocument88 pagesDisease of Biliary SystemProsanta Kr BhattacharjeeNo ratings yet
- Rheumatoid Arthritis DrugsDocument7 pagesRheumatoid Arthritis DrugsSANKET ROUTNo ratings yet
- Checklist 7 Step of Occupational Diagnosis - 2021-2022Document4 pagesChecklist 7 Step of Occupational Diagnosis - 2021-2022Putri NoviyantiNo ratings yet
- DisertasiDocument169 pagesDisertasirantiadrianiNo ratings yet
- Pain Pathways IntroductionDocument7 pagesPain Pathways Introductionganpur01100% (1)
- Avance Tramas SetiDocument47 pagesAvance Tramas SetiElvis Olivera EgasNo ratings yet
- Oral Antidiabetic DrugsDocument7 pagesOral Antidiabetic DrugsNancy ArguetaNo ratings yet
- Caregiving Lesson Quarter ExamsDocument3 pagesCaregiving Lesson Quarter ExamsGlaiza FloresNo ratings yet
- 16 Pendekatan Klinis SesakDocument36 pages16 Pendekatan Klinis SesakEks TraNo ratings yet
- LAB Test Performa (Pattern)Document3 pagesLAB Test Performa (Pattern)ripss09No ratings yet