You might also like
- Trocar Surgery for Cataract Surgeons: From Dislocated IOL to Dropped NucleusFrom EverandTrocar Surgery for Cataract Surgeons: From Dislocated IOL to Dropped NucleusNo ratings yet
- 0402 Preferred Features Cric Sets 120917Document1 page0402 Preferred Features Cric Sets 120917freemedicNo ratings yet
- 0401 Preferred Features Chest Seals 120917Document1 page0401 Preferred Features Chest Seals 120917freemedicNo ratings yet
- Technical Aspects Related to the Design and Construction of Engineered Containment Barriers for Environmental RemediationFrom EverandTechnical Aspects Related to the Design and Construction of Engineered Containment Barriers for Environmental RemediationNo ratings yet
- Tads 3mDocument10 pagesTads 3mtravolta0No ratings yet
- Keys to Successful Orthotopic Bladder SubstitutionFrom EverandKeys to Successful Orthotopic Bladder SubstitutionUrs E. StuderNo ratings yet
- Medical RobotsDocument26 pagesMedical Robotsajaygill5785No ratings yet
- Junction Box Installation Operation ManualDocument16 pagesJunction Box Installation Operation ManualMd asrar aliNo ratings yet
- Ifu Pda 2018Document12 pagesIfu Pda 2018Joresp EspinozaNo ratings yet
- DS Prestress HBDocument28 pagesDS Prestress HBBrian James MarzanNo ratings yet
- Stryker Variax Fibula OTDocument24 pagesStryker Variax Fibula OTDan IonescuNo ratings yet
- CER - OSCAR 3 - C.1.1 - Rev. 2Document101 pagesCER - OSCAR 3 - C.1.1 - Rev. 2santiago100% (1)
- Sd-06 Spray Dryer: Assembly & Operating InstructionsDocument16 pagesSd-06 Spray Dryer: Assembly & Operating Instructionsfacu_falaNo ratings yet
- Rigidloop EspañolDocument48 pagesRigidloop EspañolLUCIA SOLIS0% (1)
- Surgical RobotsDocument48 pagesSurgical RobotsRohanNo ratings yet
- 001 0956 01 Rev A Prima Cocr Ifu enDocument2 pages001 0956 01 Rev A Prima Cocr Ifu enDr. Anand RajapurNo ratings yet
- KS MNL ENG 04 01 (Retractable)Document13 pagesKS MNL ENG 04 01 (Retractable)chakrapani vagish chandra pandeyNo ratings yet
- Excro Rope Socket TesterDocument16 pagesExcro Rope Socket TesterWilliam EvansNo ratings yet
- Boston KPro Click-On ManualDocument42 pagesBoston KPro Click-On ManualHang doNo ratings yet
- Surgical Manual 2018/2019: Internal Hex & cONICAL pLATFORMDocument38 pagesSurgical Manual 2018/2019: Internal Hex & cONICAL pLATFORMmaria teresa pertuz rondonNo ratings yet
- ACCOLADE II SurgicalDocument11 pagesACCOLADE II Surgicaltrinh thanhNo ratings yet
- 2019 Recommended Limb Tourniquets in Tactical Combat Casualty CareDocument24 pages2019 Recommended Limb Tourniquets in Tactical Combat Casualty CaregelcMDNo ratings yet
- Filed Guide Audiometric Test Booth CertificationDocument4 pagesFiled Guide Audiometric Test Booth CertificationJoseph PimpolloNo ratings yet
- Transoral Surgery: Procedure GuideDocument32 pagesTransoral Surgery: Procedure GuideanisNo ratings yet
- Rees Group Senior Design ReportDocument94 pagesRees Group Senior Design Reportapi-239925747No ratings yet
- Final Brochure 2014Document20 pagesFinal Brochure 2014Annie NguyễnNo ratings yet
- Techsonic EZ III Rev 4 092010 PDFDocument70 pagesTechsonic EZ III Rev 4 092010 PDFandresgomez10No ratings yet
- Super Line Prosthesis ManualDocument50 pagesSuper Line Prosthesis Manualclaudia360No ratings yet
- Centrifuge 4Document1 pageCentrifuge 4admin ptkmiNo ratings yet
- GNATUSDocument26 pagesGNATUSAndi Sugianto75% (4)
- SuperLine and Implantium (Manual)Document50 pagesSuperLine and Implantium (Manual)Ovidiu NeculauNo ratings yet
- PROPHECY INBONE Surgical TechniqueDocument68 pagesPROPHECY INBONE Surgical TechniqueSarah GaelNo ratings yet
- Chapter 9 - Considerations Common To Mainstream Dental Implant Treatment ProtocolsDocument30 pagesChapter 9 - Considerations Common To Mainstream Dental Implant Treatment ProtocolsKomal TalrejaNo ratings yet
- Tactical Field Care 2a: (Based On TCCC-MP Guidelines 180801)Document35 pagesTactical Field Care 2a: (Based On TCCC-MP Guidelines 180801)Luis-alfredo Perez Bolde HernandezNo ratings yet
- Double Pigtail Percuflex Ureteral Stents and Stent SetsDocument38 pagesDouble Pigtail Percuflex Ureteral Stents and Stent SetscateterdoblejotaNo ratings yet
- 3 Tactical Field CareDocument164 pages3 Tactical Field CareINSTRUCTOR INTERNACIONAL ANTONIO RAMIREZNo ratings yet
- LAB 142 - Implants For Ligament & Tendon Reconstruction - Product PortfolioDocument8 pagesLAB 142 - Implants For Ligament & Tendon Reconstruction - Product PortfolioAaron RossNo ratings yet
- Implantarmamentarium 170902170115Document99 pagesImplantarmamentarium 170902170115Recep Vatansever0% (1)
- FP29811 6Document1 pageFP29811 6Nayib Ernesto Diaz GomezNo ratings yet
- IFU1062 Celosia Covered Stent Rev. BDocument11 pagesIFU1062 Celosia Covered Stent Rev. BAnnie NguyễnNo ratings yet
- Removal of Hardware BlogDocument5 pagesRemoval of Hardware BlogJill McAngusNo ratings yet
- 06 - Health and Safety Specifications - v1.0 - 20100617Document10 pages06 - Health and Safety Specifications - v1.0 - 20100617yoki_triwahyudiNo ratings yet
- VNX5300 Add IO ModuleDocument11 pagesVNX5300 Add IO ModuleLoren DiezNo ratings yet
- IST25 BWA014K - Rev 0 - 12 19Document8 pagesIST25 BWA014K - Rev 0 - 12 19EloisaNo ratings yet
- Mini-Mandible Plaitng System 2-2.5mmDocument17 pagesMini-Mandible Plaitng System 2-2.5mmHardikNo ratings yet
- Ancor ProDocument4 pagesAncor ProOrtho OrganizersNo ratings yet
- Preparation For Running CasingDocument3 pagesPreparation For Running CasingYougchu LuanNo ratings yet
- Basic Implant Surgery: Dental ImplantsDocument7 pagesBasic Implant Surgery: Dental ImplantsHau TranNo ratings yet
- 023664-160505 XCEL Bladeless Trocar Fact Sheet Final PDFDocument2 pages023664-160505 XCEL Bladeless Trocar Fact Sheet Final PDFdido fidoNo ratings yet
- Array of Robots Augmenting The Kinematics of Endocavitary SurgeryDocument9 pagesArray of Robots Augmenting The Kinematics of Endocavitary SurgeryAnjireddy ThatiparthyNo ratings yet
- 3 TFC 1-No VideosDocument135 pages3 TFC 1-No VideosMurasa2009No ratings yet
- Thesis PresentationDocument44 pagesThesis Presentationberhe59076362No ratings yet
- OPGW Installation ManualDocument35 pagesOPGW Installation ManualJoanna BaileyNo ratings yet
- PDFDocument10 pagesPDFmedgadget100% (1)
- Sd-Basic Spray Dryer Assembly & Operating InstructionsDocument9 pagesSd-Basic Spray Dryer Assembly & Operating InstructionsvinibenalNo ratings yet
- RotoBin Manual Roto-Bin-Dicator-Level-Indicator-Installation-Operation-ManualDocument16 pagesRotoBin Manual Roto-Bin-Dicator-Level-Indicator-Installation-Operation-ManualAlexandre Caique SampaioNo ratings yet
- Annex 6 Generic Specifications For X-Ray and Ultrasound UnitsDocument5 pagesAnnex 6 Generic Specifications For X-Ray and Ultrasound UnitsMirkoLopezNo ratings yet
- Safe Operating Procedure: (Revised 4/19) Personal Fall Arrest SystemsDocument7 pagesSafe Operating Procedure: (Revised 4/19) Personal Fall Arrest SystemsUlviyye ElesgerovaNo ratings yet
- A Fieldbook of The StarsDocument130 pagesA Fieldbook of The StarsLiam Glen MurdochNo ratings yet
- C TuningDocument1 pageC TuningfreemedicNo ratings yet
- C TuningDocument1 pageC TuningfreemedicNo ratings yet
- The Ukulele: A Magical History Tour: Bonus ChapterDocument2 pagesThe Ukulele: A Magical History Tour: Bonus Chapterfreemedic0% (1)
- BeretsDocument1 pageBeretsfreemedic100% (1)
- 6352 USN Phantoms in CombatDocument66 pages6352 USN Phantoms in Combatfreemedic100% (16)
- Point North CatalogDocument84 pagesPoint North CatalogfreemedicNo ratings yet
- Size of Tackle: The First Thing To Know Is What: OR LeatherDocument5 pagesSize of Tackle: The First Thing To Know Is What: OR Leatherelectricnusi100% (7)
- Preserving MeatDocument16 pagesPreserving Meatfreemedic100% (2)
- A Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentDocument6 pagesA Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentfreemedicNo ratings yet
- Department of The Army Pyrotechnics Branch Aberdeen Proving Ground, Maryland 21020-5423Document5 pagesDepartment of The Army Pyrotechnics Branch Aberdeen Proving Ground, Maryland 21020-5423freemedicNo ratings yet
- BOWIE KNIFE RevisitingBlackQuestionDocument17 pagesBOWIE KNIFE RevisitingBlackQuestionfreemedicNo ratings yet
- America S Greatest Special Ops Soldier Maj Dick MeadowsDocument7 pagesAmerica S Greatest Special Ops Soldier Maj Dick MeadowsfreemedicNo ratings yet
- Soldiers of The Napoleonic Wars #4 - Colours and Weapons - British Foot Guards at Waterloo, June 1815Document26 pagesSoldiers of The Napoleonic Wars #4 - Colours and Weapons - British Foot Guards at Waterloo, June 1815J054663100% (7)
- Joining Instructions For Improvised Explosive Device - Medical Trauma Management Course (Ied-Mtmc) Aim. The Aim of Improvised Explosive DeviceDocument2 pagesJoining Instructions For Improvised Explosive Device - Medical Trauma Management Course (Ied-Mtmc) Aim. The Aim of Improvised Explosive DevicefreemedicNo ratings yet
- Chinook Cargo SystemDocument188 pagesChinook Cargo SystemfreemedicNo ratings yet
- My Survival Gear by Tom Tindell: Flint KitDocument3 pagesMy Survival Gear by Tom Tindell: Flint Kitfreemedic100% (1)
- Preparedness List of ListsDocument5 pagesPreparedness List of Listsfreemedic100% (2)
- Alss Aircrew Life SupportDocument74 pagesAlss Aircrew Life SupportfreemedicNo ratings yet
- Chapter 14Document32 pagesChapter 14freemedicNo ratings yet
- Reference Book ListDocument4 pagesReference Book Listfreemedic0% (1)
- Camping EssentialsDocument1 pageCamping EssentialsfreemedicNo ratings yet
- Safety and SurvivalDocument4 pagesSafety and SurvivalfreemedicNo ratings yet
- US Army Camouflage Concealment and Decoys 1999Document96 pagesUS Army Camouflage Concealment and Decoys 1999Adam WardNo ratings yet
- WoodsmokeDocument2 pagesWoodsmokefreemedicNo ratings yet
- Ayaz Ahmed SoomroDocument9 pagesAyaz Ahmed SoomroNoman RathoreNo ratings yet
- 2018 2019UndergraduateEnglishTaughtCoursesDocument40 pages2018 2019UndergraduateEnglishTaughtCoursesmalu accountNo ratings yet
- Catalogo Lowara DomoDocument6 pagesCatalogo Lowara DomoSergio ZegarraNo ratings yet
- Protected Cultivation of Grapes 1623232731Document40 pagesProtected Cultivation of Grapes 1623232731Karan Bir Singh GillNo ratings yet
- Fpso Revamp For A Marginal Field Ea-SpeDocument34 pagesFpso Revamp For A Marginal Field Ea-Spe고병석No ratings yet
- Child and Adolescent LiteratureDocument21 pagesChild and Adolescent LiteratureHazel GeronimoNo ratings yet
- DownloadDocument12 pagesDownloadAdemar Espírito SantoNo ratings yet
- GPSA 2nd Phase Tender For CUIS 2021-22Document1 pageGPSA 2nd Phase Tender For CUIS 2021-22Mwandembo Ushindi0% (1)
- Freshers - HR Interview Questions at AccentureDocument3 pagesFreshers - HR Interview Questions at Accenturebtrecio03No ratings yet
- Larry Stylinson Proof.Document174 pagesLarry Stylinson Proof.arantxaNo ratings yet
- ECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Document33 pagesECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Erick Lizana Neyra100% (4)
- Advantages and Disadvantages. Personal Blogging TestDocument2 pagesAdvantages and Disadvantages. Personal Blogging TestLaura, GarciaNo ratings yet
- Tele-Directory - July-2021Document32 pagesTele-Directory - July-2021Vijay Press ConferenceNo ratings yet
- Theoretical Foundation For Large-Scale Computations For Nonlinear Material BehaviorDocument411 pagesTheoretical Foundation For Large-Scale Computations For Nonlinear Material BehaviorDalelAzaiezNo ratings yet
- Aeci Mining Explosives Product Catalogue Surface Bulk Emulsions 2019 OctoberDocument14 pagesAeci Mining Explosives Product Catalogue Surface Bulk Emulsions 2019 OctoberMohamed Badian Traore0% (1)
- Aldi and Walmart CaseDocument4 pagesAldi and Walmart CaseJackNo ratings yet
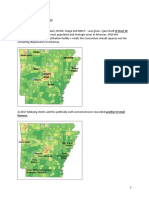
- Arkansas DispensariesDocument6 pagesArkansas DispensariesAdam ByrdNo ratings yet
- Reaction of Rhodium With AirDocument2 pagesReaction of Rhodium With AirVhandy RamadhanNo ratings yet
- Basic Electronics New - 3110016Document4 pagesBasic Electronics New - 3110016Sneha PandyaNo ratings yet
- Antimicrobial Spectrum and Characteristics of Hand-Hygiene Antiseptic AgentsDocument3 pagesAntimicrobial Spectrum and Characteristics of Hand-Hygiene Antiseptic AgentsdonsterthemonsterNo ratings yet
- Prs-021-0025 - C. Melchers - Coca Cola Naga ProjectDocument2 pagesPrs-021-0025 - C. Melchers - Coca Cola Naga ProjectMiko Christopher OroyanNo ratings yet
- Negotiable Instruments Amendment Act 2015Document6 pagesNegotiable Instruments Amendment Act 2015Latest Laws Team100% (1)
- Penilaian Kelayakan Usaha Mikro Dengan Kredit Skoring Dan Pengaruhnya Terhadap Pembiayaan Bermasalah Best Practice Lembaga Keuangan Di IndonesiaDocument12 pagesPenilaian Kelayakan Usaha Mikro Dengan Kredit Skoring Dan Pengaruhnya Terhadap Pembiayaan Bermasalah Best Practice Lembaga Keuangan Di IndonesiaRiantriaNo ratings yet
- Federico Giusfredi - Syntax of The Luwian LanguageDocument229 pagesFederico Giusfredi - Syntax of The Luwian LanguageLucySky7No ratings yet
- "Cryptochart - Cryptocurrency Price Tracker": East West College of ManagementDocument66 pages"Cryptochart - Cryptocurrency Price Tracker": East West College of ManagementSriharsha S ANo ratings yet
- Food Stuff From List CompaniesDocument3 pagesFood Stuff From List CompaniesListonNo ratings yet
- Jawaban Materi 3Document7 pagesJawaban Materi 3Aminatus MahmudahNo ratings yet
- Union Feb. 10, 2016Document16 pagesUnion Feb. 10, 2016Your News. When You Want It.No ratings yet
- Radiation Monitoring InstrumentsDocument107 pagesRadiation Monitoring InstrumentsCristina ȚărnăNo ratings yet
- Каталог гидромолот JCB HM385Document2 pagesКаталог гидромолот JCB HM385бекиров эрнестNo ratings yet