You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
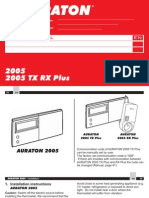
- Auraton 2005Document24 pagesAuraton 2005Muhidin KozicaNo ratings yet
- NDocument54 pagesNfieza_ajeeNo ratings yet
- Carlisle Co Elemetary IAQDocument24 pagesCarlisle Co Elemetary IAQMohd Shaharuddin Abdul LatiffNo ratings yet
- Aluminium Industry - Aluminium Du Maroc Company: Mechanical and Metallurgical Sector - MoroccoDocument2 pagesAluminium Industry - Aluminium Du Maroc Company: Mechanical and Metallurgical Sector - MoroccoMohd Shaharuddin Abdul LatiffNo ratings yet
- Indoor Air Quality Investigation (Client Name) (City, State)Document7 pagesIndoor Air Quality Investigation (Client Name) (City, State)Mohd Shaharuddin Abdul LatiffNo ratings yet
- 1 Intro Ind-HygieneDocument21 pages1 Intro Ind-HygieneMohd Shaharuddin Abdul LatiffNo ratings yet
- Company Introduction: Osaka Vacuum Chemical (Malaysia) Sdn. BHDDocument10 pagesCompany Introduction: Osaka Vacuum Chemical (Malaysia) Sdn. BHDMohd Shaharuddin Abdul LatiffNo ratings yet
- Industrial COP On IAQDocument50 pagesIndustrial COP On IAQtamanriveriaNo ratings yet
- Panduan Penulisan Laporan (Iaq)Document2 pagesPanduan Penulisan Laporan (Iaq)Mohd Shaharuddin Abdul LatiffNo ratings yet
- Indoor Air Quality and Sick Building Syndrome in Malaysian BuildingsDocument10 pagesIndoor Air Quality and Sick Building Syndrome in Malaysian BuildingsMohd Shaharuddin Abdul LatiffNo ratings yet
- Panduan Penulisan Laporan (Iaq)Document2 pagesPanduan Penulisan Laporan (Iaq)Mohd Shaharuddin Abdul LatiffNo ratings yet
- Application FormDocument2 pagesApplication FormMohd Shaharuddin Abdul LatiffNo ratings yet
- Microsoft Word - Bulletin 32005Document4 pagesMicrosoft Word - Bulletin 32005Mohd Shaharuddin Abdul LatiffNo ratings yet
- MankindDocument23 pagesMankindanandkas2005100% (1)
- Review On Metallization Approaches For High-Efficiency Silicon Heterojunction Solar CellsDocument16 pagesReview On Metallization Approaches For High-Efficiency Silicon Heterojunction Solar Cells蕭佩杰No ratings yet
- Science Investigatory ProjectDocument17 pagesScience Investigatory ProjectVhon AndreaNo ratings yet
- The Wall Street Journal - 05.01.22Document28 pagesThe Wall Street Journal - 05.01.22TIMOTEO ROJAS CARRILLONo ratings yet
- Lab ReportDocument2 pagesLab Reportapi-243032999No ratings yet
- PGFS ND 023 R0 PrimusGFS General Regulations Appendix 4 Scope Education and Work Experience PDFDocument3 pagesPGFS ND 023 R0 PrimusGFS General Regulations Appendix 4 Scope Education and Work Experience PDFGreilin CastilloNo ratings yet
- Kunft KDW4752N DishwasherDocument59 pagesKunft KDW4752N Dishwashermike_sanNo ratings yet
- OTC-26068-MS Wettability Alteration of Heavy-Oil/Bitumen Containing Carbonates Using Solvents, High PH Solutions and Nano/Ionic LiquidsDocument18 pagesOTC-26068-MS Wettability Alteration of Heavy-Oil/Bitumen Containing Carbonates Using Solvents, High PH Solutions and Nano/Ionic Liquidsjose floresNo ratings yet
- 1) Gobar Danga Model: Purpose of Visit: To IntroduceDocument6 pages1) Gobar Danga Model: Purpose of Visit: To IntroduceArun BiswasNo ratings yet
- Anti-Violence Against Women and Their Children Act of 2004 (Republic Act No. 9262)Document5 pagesAnti-Violence Against Women and Their Children Act of 2004 (Republic Act No. 9262)Tobythe BullyNo ratings yet
- Importance of Soil TextureDocument3 pagesImportance of Soil TextureindriyaniNo ratings yet
- ESWT - For Myositis Ossificans CaseDocument13 pagesESWT - For Myositis Ossificans CaseSienriesta NovianaNo ratings yet
- WSET L1 2 Wines SpecificationDocument46 pagesWSET L1 2 Wines Specificationcipollina666No ratings yet
- Reaction PaperDocument3 pagesReaction PaperMondejar KhriziaNo ratings yet
- NEOTHERM 70 EVO - 60V Manual - P1600 PDFDocument23 pagesNEOTHERM 70 EVO - 60V Manual - P1600 PDFm_armouti100% (1)
- Solar Direct-Drive Vaccine Refrigerators and Freezers: The Need For Off-Grid Cooling OptionsDocument10 pagesSolar Direct-Drive Vaccine Refrigerators and Freezers: The Need For Off-Grid Cooling OptionsRolando mendozaNo ratings yet
- Modern Power Transformer Practice - R. Feinberg PDFDocument360 pagesModern Power Transformer Practice - R. Feinberg PDFAlberto Ortiz100% (1)
- Askiitians Chemistry Test213Document10 pagesAskiitians Chemistry Test213Yusuf JamilNo ratings yet
- BHB SandeepDocument2 pagesBHB SandeepAbzad HussainNo ratings yet
- Income Tax: Global Income TaxDocument4 pagesIncome Tax: Global Income TaxMichelle Muhrie TablizoNo ratings yet
- 4 Sem C.T Unit 3 Water Cement RatioDocument4 pages4 Sem C.T Unit 3 Water Cement RatioToufiq BhatiNo ratings yet
- Study of Spray DryingDocument18 pagesStudy of Spray DryingMahe Rukh100% (2)
- Pregnancy in Dental TreatmentDocument62 pagesPregnancy in Dental TreatmentChinar HawramyNo ratings yet
- Happiness Coaching NewDocument28 pagesHappiness Coaching NewMahesh RaoNo ratings yet
- Pnoz S2 24Vdc 3 N/O 1 N/C 750102: Pilz GMBH & Co. KG, Felix-Wankel-Strasse 2, 73760 Ostfildern, Germany Page 1/3Document3 pagesPnoz S2 24Vdc 3 N/O 1 N/C 750102: Pilz GMBH & Co. KG, Felix-Wankel-Strasse 2, 73760 Ostfildern, Germany Page 1/3Ibraheem AlfalahatNo ratings yet
- Body Systems TestDocument6 pagesBody Systems TestIRENE DÁVALOS SMILGNo ratings yet
- Isagenix Isalean Shake Vs Visalus Shake 5 16 12Document8 pagesIsagenix Isalean Shake Vs Visalus Shake 5 16 12api-150110825No ratings yet
- 1.classical Conditioning TheoryDocument5 pages1.classical Conditioning TheoryNIHAR RANJAN MishraNo ratings yet
- Nutrition Through-Out Lifespan (Infancy)Document37 pagesNutrition Through-Out Lifespan (Infancy)Vincent Maralit MaterialNo ratings yet