You might also like
- 24 Emergency DrugsDocument7 pages24 Emergency DrugsApple BelicanNo ratings yet
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesFrom EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesRating: 5 out of 5 stars5/5 (1)
- CRASH CART PresentationDocument33 pagesCRASH CART PresentationSanil Thomas91% (23)
- Intravenous Therapy Administration: a practical guideFrom EverandIntravenous Therapy Administration: a practical guideRating: 4 out of 5 stars4/5 (1)
- Crash Cart Medications and ManagementDocument20 pagesCrash Cart Medications and ManagementSilpa Kuruvilla100% (2)
- Emergency Pharmacology Drugs GuideDocument5 pagesEmergency Pharmacology Drugs GuideAce RegellanaNo ratings yet
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (1)
- The Crash CartDocument39 pagesThe Crash Cartpramod kumawat100% (1)
- Emergency DrugsDocument11 pagesEmergency Drugsthenursingcorner96% (24)
- Emergency Trolley ContentsDocument28 pagesEmergency Trolley ContentsEggy Pascual100% (1)
- CRASH CART NewDocument11 pagesCRASH CART NewGemstone Dangel NdukaNo ratings yet
- Drug Study On Emergency DrugsDocument14 pagesDrug Study On Emergency Drugsjcarysuitos100% (4)
- Emergency Drugs Drug StudyDocument15 pagesEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- Common Drugs Used in The EmergencyDocument5 pagesCommon Drugs Used in The Emergencyhatem alsrour88% (25)
- Emergency DrugsDocument17 pagesEmergency Drugsapi-3853350100% (12)
- Epinephrine: Uses, Dosages, Side EffectsDocument15 pagesEpinephrine: Uses, Dosages, Side EffectsDennise Juayang100% (1)
- EMERGENCY DRUGSDocument7 pagesEMERGENCY DRUGSJohn Balgoa100% (2)
- Common Drugs Used in The Emergency RoomDocument3 pagesCommon Drugs Used in The Emergency RoomJames David Atillo Pacaña100% (5)
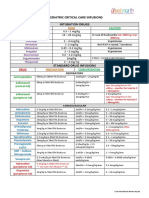
- Paediatric Critical Care Infusions Intubation DrugsDocument2 pagesPaediatric Critical Care Infusions Intubation DrugsА. Сосорбарам100% (1)
- Product Information Avil Product NamesDocument4 pagesProduct Information Avil Product Namesindyanexpress100% (1)
- CriticalCare - ICU Skills ChecklistDocument8 pagesCriticalCare - ICU Skills Checklistyash Inficare100% (2)
- Common Emergency DrugsDocument48 pagesCommon Emergency Drugshady920100% (1)
- Pre and Post Angiography and Angioplasty CareDocument34 pagesPre and Post Angiography and Angioplasty Carempimmi khanchannel50% (2)
- Hypoglycemia: Presented by Farse GhabayenDocument11 pagesHypoglycemia: Presented by Farse GhabayenFares G. Ghabayen100% (2)
- AdrenalineDocument13 pagesAdrenalineMobahil AhmadNo ratings yet
- Monthly Crash Cart InventoryDocument4 pagesMonthly Crash Cart InventoryMenGuitar100% (1)
- Drug Book On EmergencyDocument21 pagesDrug Book On EmergencyDimpal Choudhary100% (4)
- Drug Study ICUDocument15 pagesDrug Study ICUJulie Nambatac100% (1)
- Crash CartDocument55 pagesCrash Carthatem alsrour100% (4)
- Crash CartDocument12 pagesCrash CartMarcus Philip Gonzales100% (1)
- Drug Study On Emergency Drugs Final - )Document12 pagesDrug Study On Emergency Drugs Final - )wen_pil100% (3)
- Drug Study On Emergency DrugsDocument15 pagesDrug Study On Emergency DrugsCla96% (25)
- Emergency TrolleyDocument27 pagesEmergency TrolleyCully BatoksNo ratings yet
- 1 - TriageDocument44 pages1 - Triagededi fahrizalNo ratings yet
- Nurses Notes TBDocument4 pagesNurses Notes TBSanvar Mal Soni0% (2)
- Code Blue Presentation: CPR and Emergency ResponseDocument22 pagesCode Blue Presentation: CPR and Emergency ResponseNurhayatiNo ratings yet
- The ABCDE ApproachDocument4 pagesThe ABCDE Approachazmar3No ratings yet
- Sodium hyaluronate eye drops treat dry eyeDocument1 pageSodium hyaluronate eye drops treat dry eyeMichael Marquez Corpuz0% (1)
- Emergency Cart ProcedureDocument20 pagesEmergency Cart ProcedureAyiessa_AJNo ratings yet
- Hemodialysis Procedure GuideDocument2 pagesHemodialysis Procedure GuideEdRobertArnad100% (1)
- Case StudyDocument34 pagesCase StudyBSNNursing101No ratings yet
- List of Medication of Emergency TrolleyDocument1 pageList of Medication of Emergency TrolleySoon Muven100% (6)
- Should Be Available at All Sites If Feasible, Include at Sites (Not Required)Document5 pagesShould Be Available at All Sites If Feasible, Include at Sites (Not Required)Ahmed QlhamdNo ratings yet
- Steroid Tapering and Supportive Treatment Guidance V1.0Document4 pagesSteroid Tapering and Supportive Treatment Guidance V1.0NancyNo ratings yet
- ASCIA Acute Management of Anaphylaxis Guidelines 2015Document4 pagesASCIA Acute Management of Anaphylaxis Guidelines 2015tom8989No ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFDocument8 pagesASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFAyu WahyuniNo ratings yet
- Pharmacology CardiovascularDocument86 pagesPharmacology Cardiovascularamasoud96 amasoud96No ratings yet
- ACLS PharmacologyDocument6 pagesACLS PharmacologyEunice Angela Fulgueras80% (5)
- VF PediDocument6 pagesVF PedixiphoideusNo ratings yet
- ACLS ModuleDocument68 pagesACLS ModuleSalah ElbadawyNo ratings yet
- High Alert Medication EnglishDocument48 pagesHigh Alert Medication Englishassajadda lizikriNo ratings yet
- Acls STUDY GUIDE 2017Document19 pagesAcls STUDY GUIDE 2017jamesomooreNo ratings yet
- E - Cart DrugsDocument18 pagesE - Cart Drugs'SheenMarkReal'100% (2)
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- Treating Dental EmergenciesDocument15 pagesTreating Dental Emergenciesminaxi123No ratings yet
- Post Test MS RleDocument15 pagesPost Test MS RleAngel YN Patricio FlorentinoNo ratings yet
- Pharmacology of Vasopressors and InotropesDocument56 pagesPharmacology of Vasopressors and InotropesBalemlay HailuNo ratings yet
- Emergency Oxygen Therapy for Cardiac IssuesDocument11 pagesEmergency Oxygen Therapy for Cardiac IssuesMin Hong LuoNo ratings yet
- Medical Emergency in DentistryDocument42 pagesMedical Emergency in Dentistrywaseem quazi100% (3)
- Protocol for managing pesticide poisoningDocument6 pagesProtocol for managing pesticide poisoningJesicca SNo ratings yet
- NUR3111 Post-Lecture QuizDocument28 pagesNUR3111 Post-Lecture QuizliNo ratings yet
- Blood Vessels NotesDocument5 pagesBlood Vessels NotesJan Vincent GoNo ratings yet
- Heart Disease Thesis StatementDocument6 pagesHeart Disease Thesis StatementHelpWithPaperCanada100% (2)
- Nursing Care Plan for PreeclampsiaDocument2 pagesNursing Care Plan for PreeclampsiaTsu Wei Chua0% (1)
- BLS Acls Aha 2020Document103 pagesBLS Acls Aha 2020Nicholas PetrovskiNo ratings yet
- Acute Coronary SyndromeDocument46 pagesAcute Coronary Syndromewiwidhipw18No ratings yet
- Pembahasan To Online 5Document522 pagesPembahasan To Online 5vanadiel4No ratings yet
- Exercise Tolerance TestDocument15 pagesExercise Tolerance TestahmedNo ratings yet
- Textbook of GB Madhuri For Cardio-Respiratory Cardiac Surgery and Thoracic Surgery ConditionsDocument340 pagesTextbook of GB Madhuri For Cardio-Respiratory Cardiac Surgery and Thoracic Surgery ConditionsBpt4 Kims100% (1)
- YMJE 2022 ASE AbstractsDocument103 pagesYMJE 2022 ASE AbstractsGuillermo CenturionNo ratings yet
- Texas Heart Institute Journal: Fever-Induced Brugada Syndrome in Patients With Malaria Plasmodium FalciparumDocument7 pagesTexas Heart Institute Journal: Fever-Induced Brugada Syndrome in Patients With Malaria Plasmodium FalciparumJimmy JimmyNo ratings yet
- Blood Pressure-For StudentsDocument79 pagesBlood Pressure-For StudentsAshok Kumar P100% (1)
- Boardworks As Biology ContentsDocument19 pagesBoardworks As Biology ContentsStudent 365No ratings yet
- Acls Algorithms 2012Document12 pagesAcls Algorithms 2012Prashanth KumarNo ratings yet
- Pasmedicine 2019Document183 pagesPasmedicine 2019Ibrahim FoondunNo ratings yet
- Title Card Guide Card Activity Card Assessment Card Enrichment Card Tosumitup Reference Card Answer CardDocument19 pagesTitle Card Guide Card Activity Card Assessment Card Enrichment Card Tosumitup Reference Card Answer CardMyra Roa GasconNo ratings yet
- Tetralogy of FallotDocument7 pagesTetralogy of FallotAshok Kumar JangirNo ratings yet
- ECG Self Study BookDocument390 pagesECG Self Study BookChandramohan SettyNo ratings yet
- Tortora 13e Glossary 2012Document30 pagesTortora 13e Glossary 2012Shweta KhannaNo ratings yet
- ABCDE Emergency Scenarios - OSCE RevisionDocument10 pagesABCDE Emergency Scenarios - OSCE RevisionJesús AmadoNo ratings yet
- AMC BLS Training TeamDocument6 pagesAMC BLS Training TeamRajasekhar BandiNo ratings yet
- Department of Education: in Science 4 On Classroom Observation ToolDocument3 pagesDepartment of Education: in Science 4 On Classroom Observation ToolArlyne Mantillas100% (2)
- Prac Exam Style Paper 3 PDFDocument11 pagesPrac Exam Style Paper 3 PDFanubhaNo ratings yet
- ABA ABLS-Manual 08112023Document95 pagesABA ABLS-Manual 08112023chepebetosm100% (1)
- Housestaff Manual 2023-2024 - MeadeDocument267 pagesHousestaff Manual 2023-2024 - MeadeMelchor Alcántara Barrera100% (2)
- Abordaje de Paciente Con SoploDocument11 pagesAbordaje de Paciente Con SoploRigo rogerNo ratings yet
- Manual Inglês Mf9100Document45 pagesManual Inglês Mf9100pedroNo ratings yet
- Blood Pressure and SoundDocument45 pagesBlood Pressure and SoundRamanathan SunderNo ratings yet
- Proper Vital Signs MonitoringDocument7 pagesProper Vital Signs MonitoringCristoper BodionganNo ratings yet
- Muscular System PowerPointDocument12 pagesMuscular System PowerPointTeena Jacob100% (1)