You might also like
- Causative Agents Causative Agents: Headache, Myalgia, & Nausea Are Added S/SX For Streptococcal PharyngitisDocument21 pagesCausative Agents Causative Agents: Headache, Myalgia, & Nausea Are Added S/SX For Streptococcal PharyngitisDon Chiaw Manongdo100% (1)
- NCP: Chronic Obstructive Pulmonary Disease and AsthmaDocument15 pagesNCP: Chronic Obstructive Pulmonary Disease and AsthmaJavie100% (5)
- Antimonium TartaricumDocument5 pagesAntimonium TartaricumSuhas IngaleNo ratings yet
- Pharmacokinetics of Inhalation AnestheticsDocument24 pagesPharmacokinetics of Inhalation AnestheticsKinanta DewiNo ratings yet
- Upper Respiratory DisordersDocument81 pagesUpper Respiratory DisordersMaria Lyn ArandiaNo ratings yet
- Allergic RhinitisDocument1 pageAllergic RhinitisprettylittlenurseNo ratings yet
- AllergiesDocument24 pagesAllergiesCamille Joy BaliliNo ratings yet
- Diseases of The NoseDocument3 pagesDiseases of The NoseVannero SembranoNo ratings yet
- Pharm5 Common Cold EtiologyDocument5 pagesPharm5 Common Cold EtiologyChristy CorleyNo ratings yet
- Allergic RhinitisDocument24 pagesAllergic RhinitisJoshua Sitorus100% (1)
- Sinusite 3Document16 pagesSinusite 3Victor EnachiNo ratings yet
- BHN Kuliah Traumatology English Class QP-2003 BaruDocument168 pagesBHN Kuliah Traumatology English Class QP-2003 BaruazifadewiatasyaNo ratings yet
- URTDDocument61 pagesURTDfcgabasanNo ratings yet
- AllergicDocument18 pagesAllergicChethranNo ratings yet
- Pharmaco Respi1Document29 pagesPharmaco Respi1Yvonnie RosalesNo ratings yet
- Vasomotor Rhinitis IdiopatikDocument5 pagesVasomotor Rhinitis IdiopatikMuhammad Husni HutagalungNo ratings yet
- AllergiesDocument24 pagesAllergiesCamille Joy BaliliNo ratings yet
- Drugs Acting On Respiratory System 6640Document137 pagesDrugs Acting On Respiratory System 6640Umar Bakshi100% (1)
- Diagnosis of Acute Rhinitis NewDocument3 pagesDiagnosis of Acute Rhinitis NewNi Wayan Julita KpNo ratings yet
- Drugs Affecting The Respiratory SystemDocument75 pagesDrugs Affecting The Respiratory Systemone_nd_onlyuNo ratings yet
- Management of Patients With Upper Respiratory Tract DisordersDocument28 pagesManagement of Patients With Upper Respiratory Tract DisordersRuth AseriosNo ratings yet
- LaryngitisDocument11 pagesLaryngitisvirendra singhNo ratings yet
- Disease Condition: DefinitionDocument5 pagesDisease Condition: Definitionpreet kaurNo ratings yet
- Anatomy and Physiology of The NoseDocument17 pagesAnatomy and Physiology of The NoseDomz LunaNo ratings yet
- Upper Airway InfectionDocument47 pagesUpper Airway Infectionjm_john0% (1)
- ASTHMADocument5 pagesASTHMAabdulNo ratings yet
- Non-Allergic RhinitisDocument9 pagesNon-Allergic RhinitisDeden SiswantoNo ratings yet
- ENT Emergencies - DR Azwar Ridwan, SP - THT-KLDocument51 pagesENT Emergencies - DR Azwar Ridwan, SP - THT-KLHayatul AkmaLiaNo ratings yet
- Drugs Affecting The Respiratory System: Antihistamines, Decongestants, Antitussives, and ExpectorantsDocument55 pagesDrugs Affecting The Respiratory System: Antihistamines, Decongestants, Antitussives, and ExpectorantsAli Adan MohamedNo ratings yet
- Nasal Polyposis Slides 08042Document48 pagesNasal Polyposis Slides 08042Muhamad RizauddinNo ratings yet
- How To Make DiagnosisDocument16 pagesHow To Make DiagnosisayeshaNo ratings yet
- Respiratory Drugs XL Chart 3Document2 pagesRespiratory Drugs XL Chart 3cdp1587100% (1)
- Immune Disorder NotesDocument6 pagesImmune Disorder NotesMary Reigns BuhatNo ratings yet
- EPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Document34 pagesEPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Julliza Joy PandiNo ratings yet
- Asthma EditedDocument42 pagesAsthma EditedSurgicalgownNo ratings yet
- The Nose and Paranasal SinusesDocument31 pagesThe Nose and Paranasal SinusesConcepcion R. AquinoNo ratings yet
- FT-Obat Saluran NafasDocument28 pagesFT-Obat Saluran NafasdwiNo ratings yet
- Ent For General PracticeDocument46 pagesEnt For General PracticefenixaNo ratings yet
- Asthma Definition:: CausesDocument10 pagesAsthma Definition:: CausesLoly IsrainiNo ratings yet
- OutlinrDocument3 pagesOutlinrMyhen Grace QuebecNo ratings yet
- WWW Ncbi NLM Nih Gov PMC Articles PMC10371786Document25 pagesWWW Ncbi NLM Nih Gov PMC Articles PMC10371786Aditya UdawantNo ratings yet
- WEEK 9 - NCMA216 - PHARMA - Respiratory System AgentsDocument50 pagesWEEK 9 - NCMA216 - PHARMA - Respiratory System AgentsOther AccountNo ratings yet
- Respiratory Tract InfectionDocument30 pagesRespiratory Tract InfectionNaresh JoshiNo ratings yet
- Management of AsthmaDocument29 pagesManagement of AsthmaAbdullah Al ArifNo ratings yet
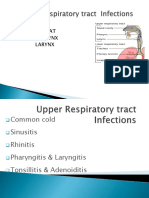
- Upper Respiratory Tract Infections 2Document87 pagesUpper Respiratory Tract Infections 2wellYONGNo ratings yet
- Chronic SinusitisDocument7 pagesChronic SinusitisMEDS easyNo ratings yet
- AsthmaDocument49 pagesAsthmaIrene AsimweNo ratings yet
- BIOGESICDocument2 pagesBIOGESICCristina FriasNo ratings yet
- Parts: Nose Throat Pharynx LarynxDocument47 pagesParts: Nose Throat Pharynx LarynxRANJIT GOGOINo ratings yet
- Group 3 Respiratory SystemDocument69 pagesGroup 3 Respiratory Systemgoodemonz15No ratings yet
- Common Diseases of PharynxDocument72 pagesCommon Diseases of PharynxPinak DeNo ratings yet
- Diseases in Children Word FileDocument12 pagesDiseases in Children Word FileLezrae Chescka Javier IlumbaNo ratings yet
- Dermatological and ENT PharmacotherapeuticsDocument16 pagesDermatological and ENT PharmacotherapeuticsOngondi TimothyNo ratings yet
- Otitis MediaDocument14 pagesOtitis MediaMelissa DavidNo ratings yet
- 2cough and ExpectationDocument37 pages2cough and ExpectationMar ClrNo ratings yet
- Asthma: History and Physical Findings: Ixsy Ramirez, MD, MPH Pediatric PulmonologyDocument32 pagesAsthma: History and Physical Findings: Ixsy Ramirez, MD, MPH Pediatric Pulmonologyfurr singhNo ratings yet
- Vertex College of Nursing Abbottabad: Hamza Ishtiaq BSN Semester 4Th Adult Health Nursing 2 DATE 09 Nov, 2018 Sir AbidDocument21 pagesVertex College of Nursing Abbottabad: Hamza Ishtiaq BSN Semester 4Th Adult Health Nursing 2 DATE 09 Nov, 2018 Sir AbidHamza IshtiaqNo ratings yet
- 11 Acute SinusitisDocument41 pages11 Acute SinusitisAshwin ParchaniNo ratings yet
- Anaphylaxis: A Practical GuideFrom EverandAnaphylaxis: A Practical GuideAnne K. EllisNo ratings yet
- Perwal PispkDocument10 pagesPerwal PispkKinanta DewiNo ratings yet
- Antibiotics in The ED How To Avoid The Common Mistake of Treating Not Wisely, But Too WellDocument32 pagesAntibiotics in The ED How To Avoid The Common Mistake of Treating Not Wisely, But Too WellKinanta DewiNo ratings yet
- Guidelines Diphtheria 2011Document21 pagesGuidelines Diphtheria 2011Kinanta DewiNo ratings yet
- Dasar Dasar Interpretasi Ekg Radityo Prakoso Hary S MuliawanDocument69 pagesDasar Dasar Interpretasi Ekg Radityo Prakoso Hary S MuliawanKinanta Dewi100% (1)
- DiphtheriaDocument6 pagesDiphtheriaKinanta DewiNo ratings yet
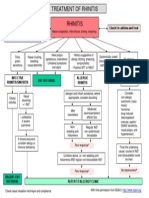
- Algorithm RhinitisPCGLDocument1 pageAlgorithm RhinitisPCGLKinanta DewiNo ratings yet
- 308 - 1 - Pentavalent Vaccine Operational Guidelines India Print Copy FinalDocument35 pages308 - 1 - Pentavalent Vaccine Operational Guidelines India Print Copy FinalKinanta DewiNo ratings yet