You might also like
- Causative Agents Causative Agents: Headache, Myalgia, & Nausea Are Added S/SX For Streptococcal PharyngitisDocument21 pagesCausative Agents Causative Agents: Headache, Myalgia, & Nausea Are Added S/SX For Streptococcal PharyngitisDon Chiaw Manongdo100% (1)
- David Lawrence CVDocument32 pagesDavid Lawrence CVM.Awais AkhterNo ratings yet
- BHN Kuliah TraumatologyDocument130 pagesBHN Kuliah TraumatologySinta Dewi AdityaniNo ratings yet
- Stopping Nasal Bleeding NaturallyDocument26 pagesStopping Nasal Bleeding NaturallyMAMA LALANo ratings yet
- Management of ENT Emergencies: Simon Lloyd Consultant ENT Surgeon Central Manchester NHS Foundation TrustDocument52 pagesManagement of ENT Emergencies: Simon Lloyd Consultant ENT Surgeon Central Manchester NHS Foundation TrustDzulkifli I. DotutinggiNo ratings yet
- URTDDocument61 pagesURTDfcgabasanNo ratings yet
- ENT Emergencies - DR Azwar Ridwan, SP - THT-KLDocument51 pagesENT Emergencies - DR Azwar Ridwan, SP - THT-KLHayatul AkmaLiaNo ratings yet
- Common Ent EmergenciesDocument65 pagesCommon Ent EmergenciesferaNo ratings yet
- Otologic, Nasal and Facial Infections GuideDocument49 pagesOtologic, Nasal and Facial Infections Guide216-104Yuda PerdanaNo ratings yet
- Epistaxis Guide: Causes, Evaluation, and ManagementDocument4 pagesEpistaxis Guide: Causes, Evaluation, and ManagementjuicyprunesNo ratings yet
- Ent For General PracticeDocument46 pagesEnt For General PracticefenixaNo ratings yet
- EpistaxisDocument39 pagesEpistaxisAbubakar JallohNo ratings yet
- Common Diseases of PharynxDocument72 pagesCommon Diseases of PharynxPinak DeNo ratings yet
- Nasal Obstruction: Meng JuanDocument36 pagesNasal Obstruction: Meng JuanReshma VasuNo ratings yet
- Rhinosinusitis: Classification, Symptoms, Diagnosis and TreatmentDocument16 pagesRhinosinusitis: Classification, Symptoms, Diagnosis and TreatmentVictor EnachiNo ratings yet
- Ent Badi PDFDocument42 pagesEnt Badi PDFsandeepNo ratings yet
- Causes, Signs, Treatment of Acute Otitis MediaDocument19 pagesCauses, Signs, Treatment of Acute Otitis MediaRajesh Sharma100% (1)
- ENT Emergencies: Stanford University Division of Emergency MedicineDocument35 pagesENT Emergencies: Stanford University Division of Emergency Medicineitho23No ratings yet
- EpistaxisDocument9 pagesEpistaxisAswathy RCNo ratings yet
- Upper Respiratory AlterationDocument34 pagesUpper Respiratory AlterationJulia ManaloNo ratings yet
- Stridor or WheezeDocument29 pagesStridor or Wheezekrishna mandalNo ratings yet
- Ear, Nose and Throat Emergencies GuideDocument4 pagesEar, Nose and Throat Emergencies GuidePenny_Teoh_3451No ratings yet
- Epistaxis: A Medical Term For A Nosebleed, Which Is A Common Presenting Complaint in The Emergency RoomDocument11 pagesEpistaxis: A Medical Term For A Nosebleed, Which Is A Common Presenting Complaint in The Emergency RoomNazurah AzmiraNo ratings yet
- DEVS Epistaxis, Septum, & Sinonasal Tumors NewwDocument24 pagesDEVS Epistaxis, Septum, & Sinonasal Tumors Newwyasin oumerNo ratings yet
- Epistaxis: A Medical Term For A Nosebleed, Which Is A Common Presenting Complaint in The Emergency RoomDocument11 pagesEpistaxis: A Medical Term For A Nosebleed, Which Is A Common Presenting Complaint in The Emergency RoomNazurah AzmiraNo ratings yet
- ENT Emergency PresentationDocument135 pagesENT Emergency PresentationshahiruddinNo ratings yet
- 4 EpistaxisDocument51 pages4 Epistaxisabhikothari30No ratings yet
- Epistaxis: Çağatay Oysu, M.D. Professor of OtolaryngologyDocument35 pagesEpistaxis: Çağatay Oysu, M.D. Professor of Otolaryngologymounes dhairyNo ratings yet
- LIMITLESS PEDIATRICS BY DR NAVEEN - DAY 4 (Green)Document56 pagesLIMITLESS PEDIATRICS BY DR NAVEEN - DAY 4 (Green)Biplav SinghNo ratings yet
- Nasal Obstruction: Nitha K 2nd Year MSC NursingDocument65 pagesNasal Obstruction: Nitha K 2nd Year MSC NursingNITHA KNo ratings yet
- Common Ent Emergencies 24126Document64 pagesCommon Ent Emergencies 24126Krittin NaravejsakulNo ratings yet
- Epistaxis Nasal Fracture Laryngeal Obstruction Gomez PedongDocument9 pagesEpistaxis Nasal Fracture Laryngeal Obstruction Gomez PedongPowell TabogocNo ratings yet
- ENT - UnitDocument63 pagesENT - Unitsuganthi rajesh kannaNo ratings yet
- Ear Nose and Throat 2Document34 pagesEar Nose and Throat 2api-195799092No ratings yet
- Epistaxis 12Document29 pagesEpistaxis 12Aryan BhatNo ratings yet
- Upper Respiratory DisordersDocument81 pagesUpper Respiratory DisordersMaria Lyn ArandiaNo ratings yet
- Upper Airway InfectionsDocument5 pagesUpper Airway InfectionsPhilline MacapagalNo ratings yet
- Throat PowerpointDocument29 pagesThroat Powerpointminci sensei100% (8)
- 09 EpistaxisDocument43 pages09 EpistaxisAbd AlsalihiNo ratings yet
- 11 Acute SinusitisDocument41 pages11 Acute SinusitisAshwin ParchaniNo ratings yet
- EPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Document34 pagesEPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Julliza Joy PandiNo ratings yet
- Epistaxis: Dr. Wachuka G. Thuku Tutorial Fellow-ENT RegistrarDocument32 pagesEpistaxis: Dr. Wachuka G. Thuku Tutorial Fellow-ENT RegistrarAlexNo ratings yet
- Drugs and Substance AbuseDocument75 pagesDrugs and Substance Abuseseline sherylNo ratings yet
- Respiratory SystemDocument24 pagesRespiratory SystemHani El-asferNo ratings yet
- S.S.Agrawal College of Nursing Training College: and Research Centre, NavsariDocument15 pagesS.S.Agrawal College of Nursing Training College: and Research Centre, NavsariPATEL NEHAKUMARI VIMALBHAINo ratings yet
- Important Topics of ENT For MBBSDocument2 pagesImportant Topics of ENT For MBBSDr.Riashat azimNo ratings yet
- Laryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDocument44 pagesLaryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDurand S. KhadkaNo ratings yet
- Acute Suppurative Otitis MediaDocument24 pagesAcute Suppurative Otitis MediaDr Tipu SultanNo ratings yet
- Diseases of Pharynx and Larynx 150406135136 Conversion Gate01Document68 pagesDiseases of Pharynx and Larynx 150406135136 Conversion Gate01dr. EndahNo ratings yet
- Common ENT ProblemsDocument41 pagesCommon ENT ProblemsMohamed GhabrunNo ratings yet
- Symptom A To Logy of EarDocument36 pagesSymptom A To Logy of Ear98480sam23006100% (1)
- 2019, Nasal Trauma and EpistaxisDocument43 pages2019, Nasal Trauma and EpistaxisakeelNo ratings yet
- Epistaxis Pic 2014 01 GDocument70 pagesEpistaxis Pic 2014 01 GJeanne d'Arc DyanchanaNo ratings yet
- MANAGEMENT OF EAR, NOSE AND THROAT DISEASESDocument16 pagesMANAGEMENT OF EAR, NOSE AND THROAT DISEASESSaurabh LamkhadeNo ratings yet
- P 3 The Upper Respiratory Tract 2Document61 pagesP 3 The Upper Respiratory Tract 2Christelle CilliersNo ratings yet
- Anatomy Head Neck EMRCS MCQDocument23 pagesAnatomy Head Neck EMRCS MCQTowhid HasanNo ratings yet
- Ch30 RespiratoryDocument18 pagesCh30 RespiratoryQuiannë Delos ReyesNo ratings yet
- 6 EpistaxisDocument19 pages6 EpistaxissuciNo ratings yet
- SinusitisDocument44 pagesSinusitisAmosNo ratings yet
- 1000 1966 1 PBDocument8 pages1000 1966 1 PBazifadewiatasyaNo ratings yet
- Protein Synthesis (Transcription and Translation) : Dr. Marhaen Hardjo, M.Biomed, PHDDocument159 pagesProtein Synthesis (Transcription and Translation) : Dr. Marhaen Hardjo, M.Biomed, PHDsNo ratings yet
- Practice Immunology SystemDocument20 pagesPractice Immunology SystemadninhanafiNo ratings yet
- Biokimia Karbohidrat Dan LemakDocument67 pagesBiokimia Karbohidrat Dan LemakazifadewiatasyaNo ratings yet
- Bab 09 Extremitas SuperiorDocument44 pagesBab 09 Extremitas Superiorsiti ayu kamsiahNo ratings yet
- Trigg Et Al 01 J Reprod Fert Suppl 57Document8 pagesTrigg Et Al 01 J Reprod Fert Suppl 57azifadewiatasyaNo ratings yet
- Progestogen-Only ContraceptivesDocument22 pagesProgestogen-Only ContraceptivesazifadewiatasyaNo ratings yet
- 068 HardonDocument10 pages068 HardonazifadewiatasyaNo ratings yet
- Primarily JHI Regarding Safe Injection Practices: Full Text Full-Text PDF (113 KB)Document4 pagesPrimarily JHI Regarding Safe Injection Practices: Full Text Full-Text PDF (113 KB)azifadewiatasyaNo ratings yet
- Essential Knowledge About Hormonal ImplantsDocument21 pagesEssential Knowledge About Hormonal ImplantsazifadewiatasyaNo ratings yet
- Contraceptive Implants: DescriptionDocument35 pagesContraceptive Implants: DescriptionazifadewiatasyaNo ratings yet
- Trigg Et Al 01 J Reprod Fert Suppl 57Document8 pagesTrigg Et Al 01 J Reprod Fert Suppl 57azifadewiatasyaNo ratings yet
- Determinants of Contraceptive Use Among Married Teenage Women and Newlywed CouplesDocument47 pagesDeterminants of Contraceptive Use Among Married Teenage Women and Newlywed CouplesazifadewiatasyaNo ratings yet
- Essential Knowledge About Hormonal ImplantsDocument21 pagesEssential Knowledge About Hormonal ImplantsazifadewiatasyaNo ratings yet
- SEXUAL DEVIANCEDocument12 pagesSEXUAL DEVIANCEazifadewiatasyaNo ratings yet
- 976 FullDocument6 pages976 FullazifadewiatasyaNo ratings yet
- Essential Knowledge About Hormonal ImplantsDocument21 pagesEssential Knowledge About Hormonal ImplantsazifadewiatasyaNo ratings yet
- 108 213 1 SMDocument7 pages108 213 1 SMazifadewiatasyaNo ratings yet
- Cost Effectiveness Analysis of Contraception Methods IUD, Injection, and Pills based on Quality of LifeDocument6 pagesCost Effectiveness Analysis of Contraception Methods IUD, Injection, and Pills based on Quality of LifeSubhan AjeNo ratings yet
- 068 HardonDocument10 pages068 HardonazifadewiatasyaNo ratings yet
- SEXUAL DEVIANCEDocument12 pagesSEXUAL DEVIANCEazifadewiatasyaNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Bathymetry and Its Applications PDFDocument158 pagesBathymetry and Its Applications PDFArseni MaximNo ratings yet
- Principles of Marketing - Product, Service and Experience DifferencesDocument26 pagesPrinciples of Marketing - Product, Service and Experience DifferencesVivien Leigh LopezNo ratings yet
- ZTE UMTS KPI Optimization Analysis Guide V1 1 1Document62 pagesZTE UMTS KPI Optimization Analysis Guide V1 1 1GetitoutLetitgo100% (1)
- Mathematical Structures of The UniverseDocument228 pagesMathematical Structures of The UniverseMaki MajomNo ratings yet
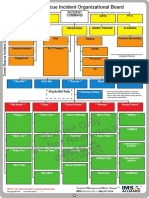
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Magellans of The Sky - Prologue - Summer 2010Document12 pagesMagellans of The Sky - Prologue - Summer 2010Prologue MagazineNo ratings yet
- MayankDocument38 pagesMayankmayank13430No ratings yet
- Logicroof V-RP enDocument1 pageLogicroof V-RP enCristina DogariNo ratings yet
- Aam April 2023Document198 pagesAam April 2023Adhitya DewantaraNo ratings yet
- 2024 Drik Panchang Telugu Calendar v1.0.1Document25 pages2024 Drik Panchang Telugu Calendar v1.0.1Sreekara GsNo ratings yet
- Singaporean Notices To Mariners: Section ContentDocument35 pagesSingaporean Notices To Mariners: Section ContentGaurav SoodNo ratings yet
- Aula 4 - Wooten - Organizational FieldsDocument28 pagesAula 4 - Wooten - Organizational FieldsferreiraccarolinaNo ratings yet
- Akbh PSK (V), TRBH As Y: AdhimokṣADocument8 pagesAkbh PSK (V), TRBH As Y: AdhimokṣA张晓亮No ratings yet
- Final Nasir GlassDocument57 pagesFinal Nasir GlassShuvo Taufiq Ahmed100% (2)
- Exercitii AdjectivDocument3 pagesExercitii AdjectivFirma GSCNo ratings yet
- High Pressure Processing For Preservation of FoodsDocument36 pagesHigh Pressure Processing For Preservation of FoodsPravin Zine PatilNo ratings yet
- Anatomy of A Plated HoleDocument5 pagesAnatomy of A Plated Holepbs0707No ratings yet
- Fundamentals of Wind EnergyDocument24 pagesFundamentals of Wind EnergyMas3odNo ratings yet
- Israel Is The MessIahDocument288 pagesIsrael Is The MessIahTeerayoot NoidaNo ratings yet
- Fitness RX For Women - December 2013Document124 pagesFitness RX For Women - December 2013renrmrm100% (2)
- Manual Bot With Relay CircuitDocument4 pagesManual Bot With Relay CircuitKarishma MishraNo ratings yet
- Actual Freedom - Made Easy (Print Friendly Edition)Document186 pagesActual Freedom - Made Easy (Print Friendly Edition)Justine100% (5)
- 3rd Periodic Test in English4Document7 pages3rd Periodic Test in English4Santa Dela Cruz Naluz100% (1)
- Cefiget-Range-Leaflet-PakistanDocument2 pagesCefiget-Range-Leaflet-PakistanZafran KhanNo ratings yet
- Capacitores Electroliticos SMDDocument8 pagesCapacitores Electroliticos SMDalvaro marrugoNo ratings yet
- Entrepreneurship Macro Environment ForcesDocument26 pagesEntrepreneurship Macro Environment ForcesSivaNo ratings yet
- Ex 2013 1 (Recurrent)Document30 pagesEx 2013 1 (Recurrent)alh basharNo ratings yet
- Understanding and Quantifying Mountain TourismDocument84 pagesUnderstanding and Quantifying Mountain TourismfloridNo ratings yet
- Edema Paru Kardiogenik Akut Kak TiaraDocument8 pagesEdema Paru Kardiogenik Akut Kak TiaraTyara LarisaNo ratings yet