You might also like
- Paul D. Purves - Cardiac Electrophysiology 2 An Advanced Visual GDocument294 pagesPaul D. Purves - Cardiac Electrophysiology 2 An Advanced Visual GAdam BarnettNo ratings yet
- The Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesDocument5 pagesThe Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesJehangir AllamNo ratings yet
- Umbilical Cord Milking PDFDocument5 pagesUmbilical Cord Milking PDFMax RodriguezNo ratings yet
- 1 Sttri 3Document6 pages1 Sttri 3parkfishyNo ratings yet
- D Farrar, A, B R Airey, C GR Law, B D Tuffnell, C B Cattle, B L DuleybDocument6 pagesD Farrar, A, B R Airey, C GR Law, B D Tuffnell, C B Cattle, B L DuleybJoseLuisTiconaNo ratings yet
- Safety of Umbilical Cord Milking in Very Preterm Neonates: A Randomized Controlled StudyDocument8 pagesSafety of Umbilical Cord Milking in Very Preterm Neonates: A Randomized Controlled StudyFatma ElzaytNo ratings yet
- Factors Influencing The Likelihood of Instrumental.11Document8 pagesFactors Influencing The Likelihood of Instrumental.11Nida Nabilah AkmalNo ratings yet
- Clampaje Tardio PDFDocument7 pagesClampaje Tardio PDFJimmy Ibañez RodriguezNo ratings yet
- Effect of Prelabour Bmi On The Mode of DeliveryDocument6 pagesEffect of Prelabour Bmi On The Mode of DeliveryIJAR JOURNALNo ratings yet
- Maternal and Newborn Outcomes Following Waterbirth: The Midwives Alliance of North America Statistics Project, 2004 To 2009 CohortDocument10 pagesMaternal and Newborn Outcomes Following Waterbirth: The Midwives Alliance of North America Statistics Project, 2004 To 2009 CohortYohanes FirmansyahNo ratings yet
- Steroid Antenatal Untuk Pengobatan Imaturitas Paru Janin Setelah 34 Minggu Usia KehamilanDocument23 pagesSteroid Antenatal Untuk Pengobatan Imaturitas Paru Janin Setelah 34 Minggu Usia KehamilanMichaela Vania TanujayaNo ratings yet
- Preterm Birth by Vacuum Extraction and Neonatal Outcome: A Population-Based Cohort StudyDocument9 pagesPreterm Birth by Vacuum Extraction and Neonatal Outcome: A Population-Based Cohort StudypfannenstielNo ratings yet
- Final Evidence Based Practice Research For Delayed Cord ClampingDocument4 pagesFinal Evidence Based Practice Research For Delayed Cord Clampingapi-498412452No ratings yet
- Insertion of An Intrauterine Contraceptive Device After Induced or Spontaneous Abortion: A Review of The EvidenceDocument6 pagesInsertion of An Intrauterine Contraceptive Device After Induced or Spontaneous Abortion: A Review of The EvidenceNi Wayan Ana PsNo ratings yet
- The Timing of Physiologic Maturation of PrematureDocument11 pagesThe Timing of Physiologic Maturation of Prematureminerva_stanciuNo ratings yet
- 26 Device Improves Swallowing in Newborns: CommentDocument33 pages26 Device Improves Swallowing in Newborns: CommentWahyuni M. Ali MreNo ratings yet
- Prognostic Factors For Successful Vaginal Birth After Cesarean Section - Analysis of 162 CasesDocument5 pagesPrognostic Factors For Successful Vaginal Birth After Cesarean Section - Analysis of 162 CasesTriponiaNo ratings yet
- Pediatrics 2012 Yee E298 304Document9 pagesPediatrics 2012 Yee E298 304Amber CarterNo ratings yet
- Risk of Respiratory Morbidity in Term Infants Delivered by Elective Caesarean Section: Cohort StudyDocument9 pagesRisk of Respiratory Morbidity in Term Infants Delivered by Elective Caesarean Section: Cohort StudyAlagendran Thanabalan PillayNo ratings yet
- NRP 7th Edition Neonatal Resuscitation GuidelinesDocument15 pagesNRP 7th Edition Neonatal Resuscitation GuidelinesAldair Cantillo BarriosNo ratings yet
- Murphy2002 Posthaemorrhagic Ventricular DilatationDocument6 pagesMurphy2002 Posthaemorrhagic Ventricular DilatationModou NianeNo ratings yet
- International Journal of Gynecology and ObstetricsDocument5 pagesInternational Journal of Gynecology and ObstetricsDewi Rahmawati SyamNo ratings yet
- Associations of Snoring Frequency and Intensity in Pregnancy With Time-To - DeliveryDocument8 pagesAssociations of Snoring Frequency and Intensity in Pregnancy With Time-To - Delivery杨钦杰No ratings yet
- Ijerph 16 00315Document16 pagesIjerph 16 00315nurlatifahNo ratings yet
- Hypothermia in Very Low Birth Weight InfantsDocument9 pagesHypothermia in Very Low Birth Weight InfantsGiovanni MictilNo ratings yet
- Transpyloric FeedingDocument10 pagesTranspyloric FeedingdryogkNo ratings yet
- Jurnal Shannaz PPHDocument17 pagesJurnal Shannaz PPHShannaz YudonoNo ratings yet
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDocument8 pagesAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyNo ratings yet
- Expectant Versus Aggressive Management in Severe Preeclampsia Remote From TermDocument6 pagesExpectant Versus Aggressive Management in Severe Preeclampsia Remote From Termmiss.JEJENo ratings yet
- Basic EcgDocument19 pagesBasic EcgIrma SihotangNo ratings yet
- No. 197b-Fetal Health SurveillanceDocument25 pagesNo. 197b-Fetal Health SurveillanceMaríaNo ratings yet
- P ('t':'3', 'I':'3053721863') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document3 pagesP ('t':'3', 'I':'3053721863') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Ni Wayan Ana PsNo ratings yet
- Pediatrics 2003 Clark 986 90Document7 pagesPediatrics 2003 Clark 986 90Giavanny Eka Rani PuteriNo ratings yet
- 2020 Delayed Vs Immediate Cord Clamping Changes Oxygen Saturation and Heart RateDocument27 pages2020 Delayed Vs Immediate Cord Clamping Changes Oxygen Saturation and Heart RatePrisaca RădășeniNo ratings yet
- Cpap Vs SurfactanteDocument10 pagesCpap Vs SurfactanteAngelicia Varela MuñozNo ratings yet
- 1233 FullDocument4 pages1233 FullMarielos Livengood de SanabriaNo ratings yet
- Care NewbornDocument17 pagesCare NewbornAndrea EusebiNo ratings yet
- Maternal and Neonatal Outcomes in Electively Induced Low-Risk Term PregnanciesDocument16 pagesMaternal and Neonatal Outcomes in Electively Induced Low-Risk Term Pregnanciessri afniNo ratings yet
- Tirado-BSN 4D-Journal Reading Summary and ReflectionDocument4 pagesTirado-BSN 4D-Journal Reading Summary and ReflectionJeniper Marie Cute29No ratings yet
- Educational Topic 32: Obstetric Procedures: U 2: O S C: PDocument4 pagesEducational Topic 32: Obstetric Procedures: U 2: O S C: PStetho LoveNo ratings yet
- Lung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFDocument8 pagesLung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFcesar juarezNo ratings yet
- Ni Hms 448407Document14 pagesNi Hms 448407Patrick RamosNo ratings yet
- 2017-Journal of Paediatrics and Child HealthDocument1 page2017-Journal of Paediatrics and Child HealthAna SopaNo ratings yet
- 2015 Neonatal Resuscitation AHADocument19 pages2015 Neonatal Resuscitation AHAJoyceAltamiranoEncisoNo ratings yet
- UC Irvine: Clinical Practice and Cases in Emergency MedicineDocument6 pagesUC Irvine: Clinical Practice and Cases in Emergency MedicinePatrick NunsioNo ratings yet
- Contemporary Cesarean Delivery Practice in The United StatesDocument17 pagesContemporary Cesarean Delivery Practice in The United StatesdedypurnamaNo ratings yet
- Obgyn 1Document4 pagesObgyn 1Auzia Tania UtamiNo ratings yet
- Jurnal Maternitas 2 EnglishDocument8 pagesJurnal Maternitas 2 EnglishmesiNo ratings yet
- Raja EA-2022Document12 pagesRaja EA-2022HAVIZ YUADNo ratings yet
- Chorioamnionitis and Prognosis For Term Infants-13Document5 pagesChorioamnionitis and Prognosis For Term Infants-13ronny29No ratings yet
- HipotermihipotermiaDocument6 pagesHipotermihipotermiaRiana Pasca RoshianNo ratings yet
- 2008 29 212 Douglas N. Carbine: Pediatrics in ReviewDocument4 pages2008 29 212 Douglas N. Carbine: Pediatrics in ReviewCraig ErkerNo ratings yet
- Vacuum Extraction in Preterm DeliveriesDocument27 pagesVacuum Extraction in Preterm DeliveriesJennifer TiosannaNo ratings yet
- Pi Is 0022347611006548Document7 pagesPi Is 0022347611006548Yudo PrabowoNo ratings yet
- Factors Predicting Survival of Growth-Restricted Babies with Absent Umbilical Artery Blood FlowDocument5 pagesFactors Predicting Survival of Growth-Restricted Babies with Absent Umbilical Artery Blood FlowdryNo ratings yet
- Prevalence of Renal Abnormalities in Infants with Urinary Tract InfectionsDocument12 pagesPrevalence of Renal Abnormalities in Infants with Urinary Tract InfectionsadipurnamiNo ratings yet
- NSVD Case Study FinalDocument60 pagesNSVD Case Study Finaljints poterNo ratings yet
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- Kidney Transplantation: A Guide to the Care of Kidney Transplant RecipientsFrom EverandKidney Transplantation: A Guide to the Care of Kidney Transplant RecipientsNo ratings yet
- Uterus TransplantationFrom EverandUterus TransplantationMats BrännströmNo ratings yet
- APA Documentation: What Is APA Style?Document13 pagesAPA Documentation: What Is APA Style?Abdulkader Mohammad KheirNo ratings yet
- EngDocument7 pagesEngmelven2jhay3No ratings yet
- Windows 8.1 KeysDocument1 pageWindows 8.1 Keysmelven2jhay3No ratings yet
- APA Format GuideDocument4 pagesAPA Format GuidefilantropiNo ratings yet
- Lenovo A369iDocument5 pagesLenovo A369imelven2jhay3No ratings yet
- Giardia SisDocument12 pagesGiardia Sismelven2jhay3No ratings yet
- MineralsDocument5 pagesMineralsmelven2jhay3No ratings yet
- Gram-Positive Rod-Shaped Anaerobic Spore-Forming Bacterium: (Formerly Known As C. Welchii, or Bacillus Welchii)Document9 pagesGram-Positive Rod-Shaped Anaerobic Spore-Forming Bacterium: (Formerly Known As C. Welchii, or Bacillus Welchii)melven2jhay3No ratings yet
- Indias Sacred CowDocument8 pagesIndias Sacred Cowmelven2jhay3No ratings yet
- Jornal Post PartumDocument4 pagesJornal Post PartumInneke DelviNo ratings yet
- Umbilical Cord Milking Improves Transition in Premature Infants at BirthDocument6 pagesUmbilical Cord Milking Improves Transition in Premature Infants at Birthmelven2jhay3No ratings yet
- Breastfeeeding BrochureDocument4 pagesBreastfeeeding Brochuremelven2jhay3No ratings yet
- How To Administer Oral Medications 1229139101116398 1Document13 pagesHow To Administer Oral Medications 1229139101116398 1melven2jhay3No ratings yet
- Borras 2019Document7 pagesBorras 2019Hill kanjinNo ratings yet
- ECG Course ECG Course: DR Rafiullah Alami MD, InternistDocument8 pagesECG Course ECG Course: DR Rafiullah Alami MD, InternistSayed AsifNo ratings yet
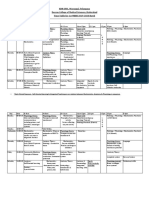
- KNRUHS 1st MBBS Time Table 2019-2020 DCMS - CumulativeDocument42 pagesKNRUHS 1st MBBS Time Table 2019-2020 DCMS - CumulativeAnime FanNo ratings yet
- Mobile Intensive Care Unit with Patient Monitor, Defibrillator and PacemakerDocument8 pagesMobile Intensive Care Unit with Patient Monitor, Defibrillator and Pacemakerwalter sandoNo ratings yet
- Universal Hospital Department of Nursing: A. Frequent Movement of The ClientDocument10 pagesUniversal Hospital Department of Nursing: A. Frequent Movement of The ClientabdallahNo ratings yet
- Datascope System 98Document16 pagesDatascope System 98Guillermo ZalazarNo ratings yet
- Ivy 101 Monitor - Service ManualDocument68 pagesIvy 101 Monitor - Service ManualcendrezNo ratings yet
- The Six Second ECG: Annotated Answer KeyDocument9 pagesThe Six Second ECG: Annotated Answer KeyShimika Tomes100% (1)
- Lecure-1 Introduction To Biomedical Instrumentation System - 4Document41 pagesLecure-1 Introduction To Biomedical Instrumentation System - 4Noor Ahmed100% (1)
- Diagnostic Procedures OverviewDocument5 pagesDiagnostic Procedures OverviewKarl KiwisNo ratings yet
- Cardiovascular SystemDocument10 pagesCardiovascular SystemitsmesuvekshaNo ratings yet
- MMP Edan M80 MS PDFDocument79 pagesMMP Edan M80 MS PDFDaniel Felipe Bello TorresNo ratings yet
- 439 3 Electrophysiology & ECG BasicsDocument34 pages439 3 Electrophysiology & ECG BasicsjpoutreNo ratings yet
- Heart Sounds, Pulse Rate, BloodDocument10 pagesHeart Sounds, Pulse Rate, Bloodkiedd_04100% (9)
- Textbook of Anaesthesia For Postgraduates PDFDocument1,218 pagesTextbook of Anaesthesia For Postgraduates PDFMohammad HayajnehNo ratings yet
- Alat Kalibrasi AccuPulseSPSDocument2 pagesAlat Kalibrasi AccuPulseSPSHermawan RevanzaNo ratings yet
- Acute Coronary SyndromeDocument43 pagesAcute Coronary SyndromeMsOrange96% (27)
- Biopotential Electrodes 1Document18 pagesBiopotential Electrodes 1cagbeko100% (1)
- 2022 Heart Screening Consent PacketDocument8 pages2022 Heart Screening Consent PacketBria GremillionNo ratings yet
- Truncus Arteriosus: Rare Heart Defect With Single Arterial TrunkDocument19 pagesTruncus Arteriosus: Rare Heart Defect With Single Arterial TrunkHijaz Al-YamanNo ratings yet
- Philippine Nursing Seminars and Training March 2011Document3 pagesPhilippine Nursing Seminars and Training March 2011PhilippineNursingDirectory.comNo ratings yet
- Bprints MEDICINE Best Copy SearchableDocument90 pagesBprints MEDICINE Best Copy SearchablePhilippe Ceasar BascoNo ratings yet
- Biomedical Instruments: Classification of Biomedical EquipmentsDocument85 pagesBiomedical Instruments: Classification of Biomedical EquipmentsDuy DươngNo ratings yet
- Detection of Cardiovascular Diseases in ECG Images Using Machine Learning and Deep Learning MethodsDocument4 pagesDetection of Cardiovascular Diseases in ECG Images Using Machine Learning and Deep Learning MethodsabhinayNo ratings yet
- ECG Clinical DemonstrationDocument24 pagesECG Clinical Demonstrationsoniya josephNo ratings yet
- AECP 1000 Augmented External Counterpulsation DeviceDocument3 pagesAECP 1000 Augmented External Counterpulsation DeviceShashidhar BhatNo ratings yet
- Conduction Blocks in AMI: A Prospective StudyDocument6 pagesConduction Blocks in AMI: A Prospective StudyJack JacksonNo ratings yet
- NCLEX Test ReviewDocument7 pagesNCLEX Test ReviewPhuong Tran100% (1)
- Modified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Document47 pagesModified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Chro MANo ratings yet