You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- FinalNurses Day MC Script - 2017Document6 pagesFinalNurses Day MC Script - 2017Luqman Hakim88% (8)
- Basic Techniques in Pediatric Surgery An Operative ManualDocument643 pagesBasic Techniques in Pediatric Surgery An Operative Manuallai chu van75% (4)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical PracticeDocument28 pagesMedical PracticeoggokNo ratings yet
- Proctoring Policy 5 12Document6 pagesProctoring Policy 5 12Dwi cahyaniNo ratings yet
- Puritani BelliniDocument291 pagesPuritani BellinioggokNo ratings yet
- Fine Art Appraisals 2013 HandoutDocument13 pagesFine Art Appraisals 2013 HandoutoggokNo ratings yet
- WHO GUIDE TO Cost-Effectiveness Analysis PDFDocument329 pagesWHO GUIDE TO Cost-Effectiveness Analysis PDFdsshhkNo ratings yet
- Evreiski Ritualni UbiistvaDocument29 pagesEvreiski Ritualni UbiistvaoggokNo ratings yet
- Lessons For Financial Success CH 5 Productivity Capacity StaffingDocument41 pagesLessons For Financial Success CH 5 Productivity Capacity StaffingoggokNo ratings yet
- Revenue Diversification ScorecardDocument2 pagesRevenue Diversification ScorecardoggokNo ratings yet
- RHC - Overseas Employment Application FormDocument5 pagesRHC - Overseas Employment Application FormspookiiNo ratings yet
- Chapter 4 - Pediatric Dentistry: Indian Health Service Dental Specialties Reference GuideDocument49 pagesChapter 4 - Pediatric Dentistry: Indian Health Service Dental Specialties Reference GuideSwastika Farah75% (4)
- Concept of Critical CareDocument11 pagesConcept of Critical CareShesly PhilominaNo ratings yet
- Daycare Safety PresentationDocument13 pagesDaycare Safety PresentationAshish KohaleNo ratings yet
- 08 01 2018 Infrastructure RegulationsDocument639 pages08 01 2018 Infrastructure Regulationsvin4343No ratings yet
- Lecture 05 - More On Modifications of Mendelian RatiosDocument2 pagesLecture 05 - More On Modifications of Mendelian RatiosRamiroCruzoNo ratings yet
- Feras Al Kharouf CVDocument3 pagesFeras Al Kharouf CVFeras Jawad AlkharoufNo ratings yet
- This Unit Group Contains The Following Occupations Included On The 2012 Skilled Occupation List (SOL)Document4 pagesThis Unit Group Contains The Following Occupations Included On The 2012 Skilled Occupation List (SOL)Abdul Rahim QhurramNo ratings yet
- Press InvitationDocument10 pagesPress InvitationPriya GokulNo ratings yet
- Category Health Workers PDFDocument37 pagesCategory Health Workers PDFAparna Kingini100% (1)
- Burns Plastic Reconstructive Surgery MSCDocument4 pagesBurns Plastic Reconstructive Surgery MSCCareer VoyageNo ratings yet
- Critical Reviews in Oral Biology & Medicine: Cementum and Periodontal Wound Healing and RegenerationDocument12 pagesCritical Reviews in Oral Biology & Medicine: Cementum and Periodontal Wound Healing and RegenerationsevattapillaiNo ratings yet
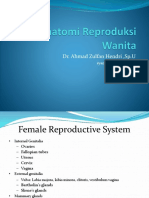
- Anatomi Reproduksi WanitaDocument23 pagesAnatomi Reproduksi WanitaocepNo ratings yet
- Aaidbonegraft09 Course Brochure PDFDocument6 pagesAaidbonegraft09 Course Brochure PDFAndria FadliNo ratings yet
- English ProficiencyDocument3 pagesEnglish ProficiencySultan AlexandruNo ratings yet
- Kim Kunzman ResumeDocument3 pagesKim Kunzman Resumeapi-280455698No ratings yet
- Obstetrics N Gynaec Nursing PDFDocument12 pagesObstetrics N Gynaec Nursing PDFSijo Muthukad M100% (1)
- Moh ExamsDocument12 pagesMoh ExamsYusuf SiddiquiNo ratings yet
- Casemix Measurement in Irish Hospitals: The Casemix Programme in Ireland - A Brief GuideDocument10 pagesCasemix Measurement in Irish Hospitals: The Casemix Programme in Ireland - A Brief GuideSaadYusufNo ratings yet
- SirkumsisiDocument15 pagesSirkumsisirizal_lutfiNo ratings yet
- Ioracon 2011 Write UpDocument6 pagesIoracon 2011 Write Upzorodocknife7354No ratings yet
- Informed Consent ORTHO TestDocument4 pagesInformed Consent ORTHO TestjohnpurdellNo ratings yet
- Reference LettersDocument8 pagesReference Lettersleonardo manabatNo ratings yet
- Neil Foley Joins NYCBS As A Physician LiaisonDocument2 pagesNeil Foley Joins NYCBS As A Physician LiaisonPR.comNo ratings yet
- Outline Clinical Response To News Triggers (With Explanatory Text) - 0 - 0 - 0Document2 pagesOutline Clinical Response To News Triggers (With Explanatory Text) - 0 - 0 - 0John SmithyNo ratings yet
- Fpdintroduction 100203103114 Phpapp02Document42 pagesFpdintroduction 100203103114 Phpapp02Sangeetha BommineniNo ratings yet
- EsicharDocument1 pageEsicharJeshiNo ratings yet