You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Kohler 5e Parts ListDocument56 pagesKohler 5e Parts ListJazzOlve75% (4)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Perlen Poesie N°33 Juin 2017 PDFDocument100 pagesPerlen Poesie N°33 Juin 2017 PDFGermaine Dupont100% (15)
- DrSueMorter The Top 3 Mistakes E Book Final 9 18 19Document28 pagesDrSueMorter The Top 3 Mistakes E Book Final 9 18 19Subash Chandar100% (8)
- Kalashtar - Eberron PathfinderDocument5 pagesKalashtar - Eberron PathfinderAenar Lith-narNo ratings yet
- Assistant Director (Environment) BPS-17Document23 pagesAssistant Director (Environment) BPS-17nomanNo ratings yet
- Monster Girl Doctor (Light Novel) Vol. 3Document237 pagesMonster Girl Doctor (Light Novel) Vol. 3pj1113069No ratings yet
- Fire Safety in High-Rise Residential BuildingsDocument17 pagesFire Safety in High-Rise Residential BuildingsDr. Yahya Mohamad Yatim75% (4)
- QA SNT Amdt 1Document2 pagesQA SNT Amdt 1raj2404No ratings yet
- Yamah F4 Owners ManualDocument70 pagesYamah F4 Owners ManualStil NoxNo ratings yet
- 2.performance and Operating Characterstics of IC EngineDocument60 pages2.performance and Operating Characterstics of IC EngineSiraj MohammedNo ratings yet
- Star Wires India LimitedDocument10 pagesStar Wires India LimitedDesh Deepak0% (1)
- GEN-CHEM-1 G11 Module3 Q1W3 MODDocument15 pagesGEN-CHEM-1 G11 Module3 Q1W3 MODDaniel Corcino100% (1)
- Pruclinicare Panel ListDocument9 pagesPruclinicare Panel ListMeng Chua60% (5)
- Hyrule Warriors - Age of Calamity - Weapons & Resources (Comments Enabled)Document20 pagesHyrule Warriors - Age of Calamity - Weapons & Resources (Comments Enabled)꧁TAKAYUKINo ratings yet
- Air Line Filter: Operating Instructions & Parts ManualDocument18 pagesAir Line Filter: Operating Instructions & Parts ManualZeckNo ratings yet
- Lab 07 Ballistic PendulumDocument3 pagesLab 07 Ballistic PendulumShahid Iltaf QureshiNo ratings yet
- The Advantages & Disadvantages of Using Biological Weapons For TerrorismDocument6 pagesThe Advantages & Disadvantages of Using Biological Weapons For TerrorismChenideNo ratings yet
- Alfiler - Class Activity No 4Document2 pagesAlfiler - Class Activity No 4Eros MadrigalNo ratings yet
- Analysis of The Essential Oils From Calendula Officinalis Growing in BrazilDocument5 pagesAnalysis of The Essential Oils From Calendula Officinalis Growing in BrazilAslı Gök-GamsızkanNo ratings yet
- Chapter-12 - Aldehydes-Ketones-and-Carboxylic-Acids Important QuestionDocument13 pagesChapter-12 - Aldehydes-Ketones-and-Carboxylic-Acids Important QuestionPonuNo ratings yet
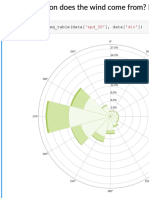
- Predicting The Wind: Data Science in Wind Resource AssessmentDocument61 pagesPredicting The Wind: Data Science in Wind Resource AssessmentFlorian RoscheckNo ratings yet
- 966f Interactivo Esquema ElectricDocument8 pages966f Interactivo Esquema ElectricJavierNo ratings yet
- 21 Test BankDocument17 pages21 Test BankNaNo ratings yet
- Relay Module, Delay Off, Off, Trigger Delay, Cycle Timing Circuit SwitchingDocument6 pagesRelay Module, Delay Off, Off, Trigger Delay, Cycle Timing Circuit SwitchingNaumaan AkkramNo ratings yet
- TS21.C11.CT01 Consolidated Test-1 On Electronic Configuration and Periodic Properties 13-06-2021 Answer KeyDocument14 pagesTS21.C11.CT01 Consolidated Test-1 On Electronic Configuration and Periodic Properties 13-06-2021 Answer KeyRAVI ANANTHAKRISHNANNo ratings yet
- Velocity: Relative Velocity of Two Bodies Moving in Straight LinesDocument5 pagesVelocity: Relative Velocity of Two Bodies Moving in Straight LinesShah IsmailNo ratings yet
- Valley View University: School of Graduate StudiesDocument13 pagesValley View University: School of Graduate Studiesvida konadu AgyemanNo ratings yet
- Ohlins - DTC - Einbauanleitung Oehlins Motorrad Ya 358Document4 pagesOhlins - DTC - Einbauanleitung Oehlins Motorrad Ya 358AsNo ratings yet
- Dallas Music Shop Zagreb CD LagerDocument174 pagesDallas Music Shop Zagreb CD Lagervjeran rukavinaNo ratings yet
- An Introduction To Polymer Physics: David I. BowerDocument29 pagesAn Introduction To Polymer Physics: David I. BowerHaseeb Zahid100% (1)