You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- GP Book Part 1 GeneralDocument45 pagesGP Book Part 1 Generalrajorshiram50% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Design Guidelines: Public & Government BuildingsDocument9 pagesDesign Guidelines: Public & Government BuildingsElisha SorianoNo ratings yet
- Nhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineDocument1 pageNhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineVadim TuscariNo ratings yet
- Paget's Disease of The Mandible - A Review and Report of A CaseDocument5 pagesPaget's Disease of The Mandible - A Review and Report of A CaseFlorin IonescuNo ratings yet
- The Importance of Macronutrients and Micronutrients in PlantsDocument25 pagesThe Importance of Macronutrients and Micronutrients in PlantsFairuz RizamNo ratings yet
- Review of The Current Status of Tooth Whitening With The Walking Bleach TechniqueDocument17 pagesReview of The Current Status of Tooth Whitening With The Walking Bleach TechniqueFlorin IonescuNo ratings yet
- JurnalDocument5 pagesJurnalSeptina Anggun PNo ratings yet
- Prognosis of Luxated Permanent Teeth - The Development of Pulp NecrosisDocument15 pagesPrognosis of Luxated Permanent Teeth - The Development of Pulp NecrosisFlorin IonescuNo ratings yet
- Periapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesDocument9 pagesPeriapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesFlorin Ionescu100% (1)
- Methods For Removing Metal Obstructions From The Root CanalDocument16 pagesMethods For Removing Metal Obstructions From The Root CanalFlorin IonescuNo ratings yet
- Mechanisms of Antimicrobial Activity of Calcium Hydroxide - A Critical ReviewDocument9 pagesMechanisms of Antimicrobial Activity of Calcium Hydroxide - A Critical ReviewFlorin IonescuNo ratings yet
- Microbial Micro Leakage and Pulpal Inflammation - A ReviewDocument8 pagesMicrobial Micro Leakage and Pulpal Inflammation - A ReviewFlorin IonescuNo ratings yet
- Intentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasDocument8 pagesIntentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasFlorin IonescuNo ratings yet
- Management of Dens Evaginatus Evaluation of Two Prophylactic Treatment MethodsDocument5 pagesManagement of Dens Evaginatus Evaluation of Two Prophylactic Treatment MethodsFlorin IonescuNo ratings yet
- Animal HusbandryDocument21 pagesAnimal HusbandryKshiteeja DushingNo ratings yet
- Ruñez, Jr. vs. JuradoDocument8 pagesRuñez, Jr. vs. JuradoEric RamilNo ratings yet
- A Progress of Herbal Finish (Aloe Vera & Neem) in Infant Tank Tops in Mother's View PointDocument6 pagesA Progress of Herbal Finish (Aloe Vera & Neem) in Infant Tank Tops in Mother's View PointEditor IJTSRDNo ratings yet
- Basic Oral Care For Patients With DysphagiaDocument9 pagesBasic Oral Care For Patients With DysphagiaAngélica GarcíaNo ratings yet
- SDS Fc-E2082taDocument8 pagesSDS Fc-E2082taPunyawich FungthongjaroenNo ratings yet
- 17CV72 - DRSS - NotesDocument57 pages17CV72 - DRSS - Notes2BL19CV065- ROJA MUJAWAR -ANo ratings yet
- The Heart and Soul of EftDocument190 pagesThe Heart and Soul of EftM Gloria-divine Turner100% (14)
- 3.6.5. One-Shot AcidDocument1 page3.6.5. One-Shot Acidpedro taquichiriNo ratings yet
- Metal 2010 Notification EnglishDocument1 pageMetal 2010 Notification EnglishNeelima VermaNo ratings yet
- Sanosil Biotech Pvt. LTD.: Material Safety Data SheetDocument7 pagesSanosil Biotech Pvt. LTD.: Material Safety Data SheetRamdas NagareNo ratings yet
- Chemical Fact SheetDocument2 pagesChemical Fact SheetAnonymous dp5b3X1NANo ratings yet
- Making Brands Matter in Turbulent Times:: How To Steer Brands Through A CrisisDocument31 pagesMaking Brands Matter in Turbulent Times:: How To Steer Brands Through A Crisischiranjeeb mitraNo ratings yet
- Introduction To Pediatric DentistryDocument23 pagesIntroduction To Pediatric Dentistrydr parveen bathla0% (1)
- Nursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermDocument4 pagesNursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermErika Danalle ArceoNo ratings yet
- CHAPTER 2 - Models of HealthDocument23 pagesCHAPTER 2 - Models of HealthLalita A/P AnbarasenNo ratings yet
- Peak Flow Meter 3Document7 pagesPeak Flow Meter 3Anushree DatarNo ratings yet
- Community Wishbook 2019-2020Document40 pagesCommunity Wishbook 2019-2020Darlyn ReddyNo ratings yet
- Wipro Limited Karan 13Document15 pagesWipro Limited Karan 13Kinjal BhanushaliNo ratings yet
- Method StatementDocument4 pagesMethod StatementDebraj RoyNo ratings yet
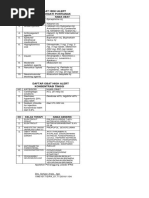
- Daftar Obat High Alert - FIXDocument2 pagesDaftar Obat High Alert - FIXDonny HartawinataNo ratings yet
- 10026-4 VHP - Packaging - Guide - 6-12-17Document226 pages10026-4 VHP - Packaging - Guide - 6-12-17DIego100% (3)
- Guide To Skilled Migration To Australia ++ Phil - Uplaw - BookDocument7 pagesGuide To Skilled Migration To Australia ++ Phil - Uplaw - BookShierwin ManabatNo ratings yet
- Nursing Management Offirst Second Stage of LaborDocument10 pagesNursing Management Offirst Second Stage of LaborSana RazaNo ratings yet
- Wk3 Slideshow Acute Responses To ExerciseDocument19 pagesWk3 Slideshow Acute Responses To Exercisejademcmahon0210100% (2)
- MBBS Private CollegeDocument3 pagesMBBS Private Collegesakif sNo ratings yet
- Refractive Error 050115Document34 pagesRefractive Error 050115Anonymous l2Fve4PpDNo ratings yet