You might also like
- Dwnload Full Neonatal and Pediatric Respiratory Care A Patient Case Method 1st Edition Perretta Test Bank PDFDocument36 pagesDwnload Full Neonatal and Pediatric Respiratory Care A Patient Case Method 1st Edition Perretta Test Bank PDFhenrywhitepw100% (11)
- Copd NCPDocument16 pagesCopd NCPSuperMaye100% (1)
- BIO121 Chapter 7 Releasing Chemical EnergyDocument45 pagesBIO121 Chapter 7 Releasing Chemical EnergyggttettanNo ratings yet
- NCP BronchopneumoniaDocument8 pagesNCP BronchopneumoniaCrisantaCasliNo ratings yet
- NCP - Poststreptococcal GlomerulonephritisDocument12 pagesNCP - Poststreptococcal GlomerulonephritisAya BolinasNo ratings yet
- Pediatric Nursing Care Plan Impaired Physical MobilityDocument5 pagesPediatric Nursing Care Plan Impaired Physical Mobilityapi-3077327050% (1)
- NCP Ineffective Airway ClearanceDocument1 pageNCP Ineffective Airway ClearanceImation DataNo ratings yet
- Actual Nursing Care Plan 2Document16 pagesActual Nursing Care Plan 2Alyanna Evangelista100% (2)
- NCP Pleural EffusionDocument7 pagesNCP Pleural EffusionEjie Boy Isaga100% (2)
- FDARDocument33 pagesFDARMiguelito Galagar Gultiano100% (2)
- Most Common Used FDAR For Ortho WardDocument19 pagesMost Common Used FDAR For Ortho WardMiguelito Galagar Gultiano75% (4)
- NcpsDocument1 pageNcpslaehaaaNo ratings yet
- Nursing Care PlanDocument15 pagesNursing Care PlanZhel Geron MercadoNo ratings yet
- Impaired Gas Exchange Pneumonia Nursing Care PlanDocument1 pageImpaired Gas Exchange Pneumonia Nursing Care Planjustin_saneNo ratings yet
- NCP - ERDocument5 pagesNCP - ERAnnelore ArcayNo ratings yet
- NCP #2Document4 pagesNCP #2Nutz TolentinoNo ratings yet
- Multi Noduar Colloid GoiterDocument1 pageMulti Noduar Colloid GoiterVincent John Faller100% (1)
- Assessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Expected OutcomeDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Expected OutcomeIsabel Barredo Del MundoNo ratings yet
- Nursing Care Plan FinalDocument16 pagesNursing Care Plan FinalErickson OcialNo ratings yet
- Activity Intolerance NCPDocument6 pagesActivity Intolerance NCPDoo NahNo ratings yet
- ARDSDocument18 pagesARDSChurrizo IslamiNo ratings yet
- B IngDocument8 pagesB IngFikriNo ratings yet
- Impaired Gas Exchange - NCPDocument4 pagesImpaired Gas Exchange - NCPJaye DangoNo ratings yet
- University of Baguio School of Nursing: Case AnalysisDocument7 pagesUniversity of Baguio School of Nursing: Case AnalysisLovely CacapitNo ratings yet
- Oxygen Administration ScriptDocument2 pagesOxygen Administration ScriptTyn TynNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataDocument2 pagesAssessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataCheila CruzNo ratings yet
- NCP JulieDocument14 pagesNCP JulieJulie Mae RubioNo ratings yet
- Assessment Nursing Diagnosis Rationale Planning Intervention/S Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Rationale Planning Intervention/S Rationale EvaluationRachel Anne Ascaño-DavidNo ratings yet
- 6w Concept MapDocument1 page6w Concept Mapapi-314635911100% (1)
- Neonatal Sepsis NCPDocument9 pagesNeonatal Sepsis NCPHollan Galicia100% (1)
- Competencymr McdougalcopdDocument17 pagesCompetencymr Mcdougalcopdmac_rymrt7569No ratings yet
- Ineffective Airway ClearanceDocument6 pagesIneffective Airway Clearanceapi-252726911No ratings yet
- NCP - Impaired Gas ExchangeDocument1 pageNCP - Impaired Gas ExchangeRryje Salleva100% (1)
- NCP Luka BakarDocument7 pagesNCP Luka BakarArian SuryaNo ratings yet
- Nursing Care Ineffective Airway Clearance: Arranged byDocument9 pagesNursing Care Ineffective Airway Clearance: Arranged byAlri LestariNo ratings yet
- Case NCPDocument25 pagesCase NCPJoher Bolante Mendez100% (1)
- PhChem 421 ManualDocument70 pagesPhChem 421 ManualSomethingSomething SomethingNo ratings yet
- Nursing Care Plan3Document6 pagesNursing Care Plan3Kristine Artes AguilarNo ratings yet
- اساسياات تمريضDocument33 pagesاساسياات تمريضHasan A AsFourNo ratings yet
- CHIEF COMPLAINTS: - Difficulty of BreathingDocument61 pagesCHIEF COMPLAINTS: - Difficulty of BreathingjonelloveuvarnalNo ratings yet
- Case Analysis 4 GERDDocument12 pagesCase Analysis 4 GERDCJ100% (1)
- Cough AsthamDocument15 pagesCough AsthamOM BAWNENo ratings yet
- Problem: Data A 68-Year-Old Man Was Admitted To The Hospital For Severe Shortness of BreathDocument1 pageProblem: Data A 68-Year-Old Man Was Admitted To The Hospital For Severe Shortness of BreathSiti nur Kholifatus samsiyahNo ratings yet
- School of Nursing and Allied Medical Sciences: Holy Angel UniversityDocument19 pagesSchool of Nursing and Allied Medical Sciences: Holy Angel UniversityMonica BorjaNo ratings yet
- Chapter 23 Clinical Review QuestionsDocument1 pageChapter 23 Clinical Review QuestionsLidia DominguezNo ratings yet
- NCP BaiaeDocument7 pagesNCP BaiaeJonathan Delos ReyesNo ratings yet
- New Born NCPDocument8 pagesNew Born NCPCarl Vincent Marrion Rejuso100% (1)
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaKahMallari100% (10)
- Nursing Care PlanDocument4 pagesNursing Care PlanKoleen KirstenNo ratings yet
- 1 Ineffective Airway ClearanceDocument8 pages1 Ineffective Airway ClearanceEsel Mae DinamlingNo ratings yet
- Nursing Care Plan Problem: Difficulty of BreathingDocument5 pagesNursing Care Plan Problem: Difficulty of BreathingIvan Louise Fajardo ManiquizNo ratings yet
- NCPPPDocument4 pagesNCPPPShane DamianNo ratings yet
- 4 NCP's FinalDocument9 pages4 NCP's FinalZenel Yap100% (1)
- NCP PTBDocument2 pagesNCP PTBKath TalubanNo ratings yet
- NCP - Impaired Gas ExchangeDocument2 pagesNCP - Impaired Gas Exchangejanelee2824No ratings yet
- Nursing Diagnosis For Imperforated AnusDocument1 pageNursing Diagnosis For Imperforated AnusAndrea Huecas Tria80% (5)
- Makalah "Pengkajian Keperawatan Pada Pasien Dan Keluarganya"Document7 pagesMakalah "Pengkajian Keperawatan Pada Pasien Dan Keluarganya"Anggi Widya LestariNo ratings yet
- Case Presentation PDFDocument59 pagesCase Presentation PDFMark EvangelioNo ratings yet
- Modl 1Document18 pagesModl 1Resty Ruslan Teke MarolaNo ratings yet
- COPDDocument47 pagesCOPDMegha VadanereNo ratings yet
- Nursing ManagementDocument16 pagesNursing ManagementNica Marie LumbaNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- A Simple Guide to Oxygen Therapy, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Oxygen Therapy, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Drug Name: - : Classification Mode of Action Side Effects Nursing ResponsibilitiesDocument2 pagesDrug Name: - : Classification Mode of Action Side Effects Nursing ResponsibilitiesMiguelito Galagar GultianoNo ratings yet
- Drug NameDocument2 pagesDrug NameMiguelito Galagar GultianoNo ratings yet
- Drug NameDocument2 pagesDrug NameMiguelito Galagar GultianoNo ratings yet
- Drug Name: - : Classification Mode of Action Side Effects Nursing ResponsibilitiesDocument2 pagesDrug Name: - : Classification Mode of Action Side Effects Nursing ResponsibilitiesMiguelito Galagar GultianoNo ratings yet
- References WBCDocument2 pagesReferences WBCMiguelito Galagar GultianoNo ratings yet
- Divalproex SODIUMDocument13 pagesDivalproex SODIUMMiguelito Galagar GultianoNo ratings yet
- CHAPTER 5 Nursing Care PlanDocument5 pagesCHAPTER 5 Nursing Care PlanMiguelito Galagar GultianoNo ratings yet
- Stimulate Renin Release: Decreased Blood Flow To O2 KidneyDocument2 pagesStimulate Renin Release: Decreased Blood Flow To O2 KidneyMiguelito Galagar GultianoNo ratings yet
- Intraop & PostopDocument63 pagesIntraop & PostopMiguelito Galagar GultianoNo ratings yet
- ABADINGO-Pedia Nursing Care PlanDocument3 pagesABADINGO-Pedia Nursing Care PlanAndrea Abadingo100% (1)
- SPS Science F3 01 PDFDocument13 pagesSPS Science F3 01 PDFMac SensNo ratings yet
- Cellular Respiration and PhotosyntesisDocument32 pagesCellular Respiration and PhotosyntesisTifahNo ratings yet
- Pangpangdeo Shanne Delle B. - Worksheet 5 ArdsDocument7 pagesPangpangdeo Shanne Delle B. - Worksheet 5 ArdsPANGPANGDEO Shanne Delle B.No ratings yet
- RespiratoryDocument16 pagesRespiratorymmacalos17735No ratings yet
- Ventilador Mekics PDFDocument4 pagesVentilador Mekics PDFBalam CaballeroNo ratings yet
- MKSAPDocument2 pagesMKSAPShaz ChindhyNo ratings yet
- Ojas Pranayam - KrishanjiDocument3 pagesOjas Pranayam - KrishanjiraychoslanchevNo ratings yet
- Flail Chest ReportDocument4 pagesFlail Chest ReportMiggsNo ratings yet
- Biological Oxidation ETCDocument37 pagesBiological Oxidation ETCsanofazal786No ratings yet
- Parañaque Science High Schoo1Document3 pagesParañaque Science High Schoo1lapNo ratings yet
- Respiratory Disease Anatomy and Phys Sheridan CollegeDocument7 pagesRespiratory Disease Anatomy and Phys Sheridan CollegeAudrey AndinoNo ratings yet
- COPD PathophysioDocument1 pageCOPD Pathophysionanette flores dela cruzNo ratings yet
- Chest TraumaDocument23 pagesChest TraumaMutaz DredeiNo ratings yet
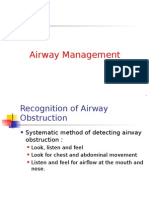
- Airway Management Recognition of Airway ObstructionDocument31 pagesAirway Management Recognition of Airway ObstructionMuhammad Hadyan RusinNo ratings yet
- Artificial RespirationDocument14 pagesArtificial RespirationDJ PNo ratings yet
- Group 2 Cardiovascular and Respiratory System of GymnastDocument19 pagesGroup 2 Cardiovascular and Respiratory System of GymnastSariephine Grace ArasNo ratings yet
- Respiratory SystemDocument19 pagesRespiratory SystemayuNo ratings yet
- Skills Laboratory 3B (Ett Suctioning) End of Rotation EvaluationDocument4 pagesSkills Laboratory 3B (Ett Suctioning) End of Rotation EvaluationmnchyNo ratings yet
- Oxygen Delivery: Franz Josef TariganDocument57 pagesOxygen Delivery: Franz Josef TariganFranz TariganNo ratings yet
- Trauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSDocument52 pagesTrauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSMariSstan EM HaNo ratings yet
- Meconium Aspiration Syndrome & Transient Tachypnea of The NewbornDocument20 pagesMeconium Aspiration Syndrome & Transient Tachypnea of The NewbornArianne AlaveNo ratings yet
- Adjusting Ventilator SettingsDocument7 pagesAdjusting Ventilator SettingsSiva RamanNo ratings yet
- Glycolysis: Cellular Respiration Cells CytoplasmDocument4 pagesGlycolysis: Cellular Respiration Cells CytoplasmArav PatelNo ratings yet
- Control of RespirationDocument15 pagesControl of RespirationChloe Gotera100% (1)
- Chemical Reaction:: Equation For Cellular Respiration C6H12O6 + O2 Co2 + H2O + E (E Stands For ATP)Document2 pagesChemical Reaction:: Equation For Cellular Respiration C6H12O6 + O2 Co2 + H2O + E (E Stands For ATP)honeylet tayactacNo ratings yet
- The Causes of An Opacified Hemithorax - KevinDocument17 pagesThe Causes of An Opacified Hemithorax - KevinKevin SurjadiNo ratings yet
- Breathing Process PDFDocument3 pagesBreathing Process PDFDianeNo ratings yet